Please remember that the following was on request, several requests actually. Also, this is blunt. It is intended to be blunt.
When is it OK to post your BFP announcement on this board, instead of going directly to PGAL and posting your announcement/intro there? Good question. Back in August, NoahBear wrote a lovely post for the blog that covered the subject well, and gave gentle guidance that relied on people's common sense.
www.ttcalblog.blogspot.com/2011/08/to-post-or-not-to-post-bfp-story.html
Prior to and since that time, there was a struggle on the board. Frankly, it got ugly. Many people who had been part of a core group of support here left under nasty suggestions that this board be 'controlled by and for newbies only', and anyone who had been here for more than 6 months should just leave. It was even suggested that they 'go back to m/c-loss' if they couldn't be happy for a random fly-by posting a 'Squeeee! I'm KTFU!' on the board.
Those sorts of suggestions were vicious and terribly painful to women who had been giving support and guidance to others and rarely asking for any themselves for a very long time. They were the glue that holds us together and provides continuity to our community. Only some of those lovely ladies who were hurt have come back. And of course, almost every single one of the women who wanted the oldies to leave have graduated and moved on. Because that's how this works. Most of you will be graduated and moved on in a few months.
However, one good thing that happened during all that, was that after almost a year of back and forth struggles trying to make this board a more supportive place (without becoming the puppies and rainbows barfing hell of babygaga.com), we found common ground and agreed upon certain ideas about posting (and graduate participation). After a few weeks, the first BFP post came and everyone held their breath. Then, only happy 'Congrats!' came and were from both newbies and oldies. Then another and another and another. Graduates felt free to come and post support for us, and no longer felt kicked out and rejected by us. Our community began to repair itself.
In time like an occasional hailstone in the rain, we noticed a few absolute newbies who had only posted for less than a month start to post BFPs. But, not wanting to bring back the all out nastiness from the past, people let them slide. Then there were a few call outs posted, the ONE sacrifice everyone had agreed on in order to find peace. But, when PSAs were posted reminding people that call outs were a no-no, the response back was 'Oh yeah? Well, the Rules aren't in the blog!' When a very new person found success on her first cycle in TTCAL, left for a few days, and then came back to post a BFP, and it was pointed out that it felt like a 'neener neener' post, the response back was 'Oh yeah? Well, the Rules aren't in the blog!'
Well. Now the 'Rules' are in the blog.
Whereas before it was left to your common sense, now it's spelled out. There is still some room for interpretation of course, we aren't toddlers, or at least we're not supposed to act like it.
Etiquette for Posting BFPs on TTCAL
1) If you are fortunate enough to find success on your first cycle or two on TTCAL, it's a pretty good bet that you should go directly to PGAL and post a BFP/Intro post there. The board as a whole hasn't yet had the chance to really get to know you or your struggles. Their happiness for your success is likely to be overshadowed by their pain of seeing yet another newb flash through and leave them behind. Posting now would only serve to hurt others. PGALers will be excited for you and welcome you with open arms. (Of course, if you were here giving support for months while you were TTA before you were TTC, then of course you've been here long enough.) Do remember that when you move over from m/c-loss you may move over with a group of women you know and feel comfortable with, but that doesn't mean that the rest of the women on TTCAL know you yet.
2) If you've been here actively giving support 3-6 cycles, and participating in the board as a member of the community, post that bad boy BFP up! If you read posts but don't respond to very many, or if you just start your own threads and don't reply much to others, then this doesn't apply to you. If in doubt, review your posting history. If the entire first page of history is all on TTCAL, all recent, and almost entirely support to others posts, you're probably fine.
3) If you're a member of 6+, then you get to post your BFP without thought or worry about it. You've been providing support and knowledge to 'generations' of TTCALers long after all your questions were answered for you by others. You've earned it. (But that's rather the point isn't it? BFPs are intended to celebrate the long-awaited success of our friends who have struggled.)
4) BFP posts should include a 'bfp warning' in the title. If you've already included a ticker in your siggy as fast as all that, please put a 'ticker warning' in the title. For reference, most graduates who post a BFP (or intend on coming back and offering support) chose not to use a ticker for a while, or use a typographic ticker ("my baby's progress"), instead of a graphical one (i.e. the fruit ticker or pictures of the developing embyo). Only graphical tickers should need warnings on BFPs. Graduates with tickers of any kind are always welcome to participate of posts started by people with 'PGAL/PAL Welcome' in their siggies, no warning needed.
5) Call out posts are absolutely not cool on this board. If you are so excited and happy for someone that you don't feel posting your comments in the OPs BFP post with everyone else is good enough for you, send a PM or call them out on PGAL (you do know that they read through those congratulation replies over, and over, and over again, right? Yours wouldn't go unnoticed. Really.). But the 'call out' posts were the price we paid for board peace. This isn't about being mean to you, it's about NOT being cruel to women who are hurting. Getting your umpteenth BFFN and logging on to TTCAL looking for support because you are losing hope seems pointless if the first page is all call outs for the latest graduate to leave you in the dust.
6) If you are new to the board, and someone is called out for their BFP post and you think it's uncalled for, perhaps you should stop, listen, and learn before condemning the very women who you will be seeking support and knowledge from, before criticizing them for calling someone out for an inappropriate post. If you are unlucky enough to be here for more than a few months, you'll figure it out fairly quickly.
7) Always remember that the intention of these rules are to provide a reminder about etiquette. Etiquette is not something to make yourself feel good, it's to make others feel good.
~Written by Petra from TTCAL


Awesome New Pregnancy Test and SALE!
Eearly-Pregnancy-Tests.com is offering a sale in excitement for a new pregnancy test.
One that allows you to see how much hcG is in your system!
Too good to be true? Maybe. I'll remain skeptical but optimistic.

One that allows you to see how much hcG is in your system!
Too good to be true? Maybe. I'll remain skeptical but optimistic.



To Post or Not To Post- A BFP Story
When new members come to the board, it's often asked "do I post my BFP here?"
Long ago, there was a time when all BFP's were welcomed if you were an active member of the community. For a while that seemed to be gone and absolutely no BFP's were "allowed". Recently, it's gone back to those who are active members can post them.
So why is the debate always coming up? That's a very good question, and no matter the answer, it wont matter. This debate will arise every few months, get heated and die down. There will be clicky polls, unpopular opinions and arguments.
A couple suggestions before you think of posting your positive pregnancy test for all to see:
-Have you supported others and somewhat gotten your "name" out there?
-Have you put a "warning" in your title (ie. pg mentioned, bfp mentioned)
-Would you consider yourself a regular on the board?
If you have to ask yourself, or others, if you're a regular, you probably aren't. If you have posted on the board, either new post or responding, a small handful of times over several months, you're probably not recognized. We don't know if you read every single post and just don't post. We don't know you until you let us. Intro, participate, support, post random things, just get out there and get your name known.
Give support, get support. Simple as that.
Long ago, there was a time when all BFP's were welcomed if you were an active member of the community. For a while that seemed to be gone and absolutely no BFP's were "allowed". Recently, it's gone back to those who are active members can post them.
So why is the debate always coming up? That's a very good question, and no matter the answer, it wont matter. This debate will arise every few months, get heated and die down. There will be clicky polls, unpopular opinions and arguments.
A couple suggestions before you think of posting your positive pregnancy test for all to see:
-Have you supported others and somewhat gotten your "name" out there?
-Have you put a "warning" in your title (ie. pg mentioned, bfp mentioned)
-Would you consider yourself a regular on the board?
If you have to ask yourself, or others, if you're a regular, you probably aren't. If you have posted on the board, either new post or responding, a small handful of times over several months, you're probably not recognized. We don't know if you read every single post and just don't post. We don't know you until you let us. Intro, participate, support, post random things, just get out there and get your name known.
Give support, get support. Simple as that.
Can It Be Genetic?
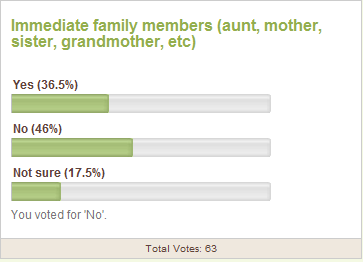
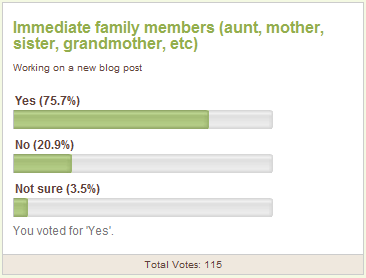
It's widly "known" that losses are not genetic. Doctors say there is no way that the trait can be passed down from either parent. Yet, when you ask the board if any of their immediate family members have had a loss, more say yes than no.
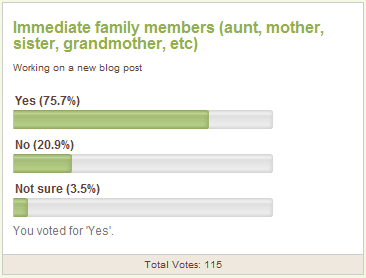
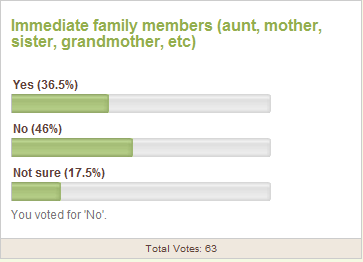
Interestingly, though, more say no than yes when it comes to infertility (secondary or initially) with a good chunk unsure.
The top Google searches when you type in "Are miscarriages...." pops up with genetic and hereditary. That's not a coincidence.
Once you've had a loss, you know how much it's out there, like a new world has been exposed. But why does it seem to pop up a lot in your own family?
Searching online and talking to doctors seem to bring up nothing. They'll say it's a fluke, a genetic abnormality (of your LO, not you) or that it's just a coincidence. There seem to have been no true studies into why they seem prevalent in families.
Perhaps one day,family losses will be a factor into your monitoring during your own pregnancy. Maybe it will help to boost your check-ins or ultrasounds or even just your betas.
Until then, we'll keep on keepin on.
Interesting articles to read:
Way Of Predicting Outcome Of Pregnancies With Miscarriage Threat Developed
Are Miscarriages Hereditary? A question on AllExperts.com
Multiple Miscarriages Linked To Gene- from 2001
Interestingly, though, more say no than yes when it comes to infertility (secondary or initially) with a good chunk unsure.
The top Google searches when you type in "Are miscarriages...." pops up with genetic and hereditary. That's not a coincidence.
Once you've had a loss, you know how much it's out there, like a new world has been exposed. But why does it seem to pop up a lot in your own family?
Searching online and talking to doctors seem to bring up nothing. They'll say it's a fluke, a genetic abnormality (of your LO, not you) or that it's just a coincidence. There seem to have been no true studies into why they seem prevalent in families.
Perhaps one day,family losses will be a factor into your monitoring during your own pregnancy. Maybe it will help to boost your check-ins or ultrasounds or even just your betas.
Until then, we'll keep on keepin on.
Interesting articles to read:
Way Of Predicting Outcome Of Pregnancies With Miscarriage Threat Developed
Are Miscarriages Hereditary? A question on AllExperts.com
Multiple Miscarriages Linked To Gene- from 2001
Save 10% at Early-Pregnancy-Tests.com
Pregnancy and Ovulation Tests:
Testing for ovulation and pregnancy at-home can be easy, quick, and 99% accurate with our tests! Determine when your ovulating by detecting you lh surge and then begin testing for pregnancy 7-10 days past ovulation.
Purchase our tests now and save 10%!
Use coupon code: ovagraph
You can also use the code to get 10% off of an OvaCue Fertility Monitor and the Spermcheck Fertility Test.
Here's a great article on using an Ovulation Predictor Kit as a Home Pregnancy test (provided by E-P-T.com)
If you are a super savvy TTC-er, you have probably heard about women using their OPKs (ovulation predictor kits) as pregnancy tests. On the other hand, if you are new to the TTC community, you might be wondering how this is possible. While it is certainly possible to use an ovulation test as a pregnancy test, it is not necessarily the most advisable method for testing for pregnancy. Here is the low-down on using an ovulation test as a pregnancy test:
An ovulation test works by detecting the surge in luteinizing hormone (LH) that precedes ovulation. Pregnancy tests work by detecting the presence of human chorionic gonadotropin (hCG) in your urine. Interestingly, hCG and LH are both known scientifically as glycoproteins, which simply means that these hormones are made up of a protein with a sugar attached to it. Of even greater interest for this discussion, is the fact that the protein parts of hCG and LH look very similar. So similar, in fact, a standard ovulation test (OPK) is unable to distinguish between LH and hCG in your urine. Therefore, if you have enough of either of the two hormones (LH or hCG) in your urine at the time you test using an OPK, you will get a positive result on the OPK.
In theory, therefore, a positive result on an ovulation test taken after you have missed a period could definitely indicate that you are pregnant. But, while it might be tempting to use your extra ovulation test as a pregnancy test, most OPKs are not as sensitive as an early detection pregnancy test, which means that you will run the risk of getting a false negative...so, even if you are pregnant, your OPK will not be sensitive enough to detect the small amounts of hCG that are present in your urine in the first few days after conception. If you suspect that you have conceived, the quickest, most accurate way to confirm pregnancy is to use an early detection pregnancy test.
Testing for ovulation and pregnancy at-home can be easy, quick, and 99% accurate with our tests! Determine when your ovulating by detecting you lh surge and then begin testing for pregnancy 7-10 days past ovulation.
Purchase our tests now and save 10%!
Use coupon code: ovagraph
You can also use the code to get 10% off of an OvaCue Fertility Monitor and the Spermcheck Fertility Test.
Here's a great article on using an Ovulation Predictor Kit as a Home Pregnancy test (provided by E-P-T.com)
If you are a super savvy TTC-er, you have probably heard about women using their OPKs (ovulation predictor kits) as pregnancy tests. On the other hand, if you are new to the TTC community, you might be wondering how this is possible. While it is certainly possible to use an ovulation test as a pregnancy test, it is not necessarily the most advisable method for testing for pregnancy. Here is the low-down on using an ovulation test as a pregnancy test:
An ovulation test works by detecting the surge in luteinizing hormone (LH) that precedes ovulation. Pregnancy tests work by detecting the presence of human chorionic gonadotropin (hCG) in your urine. Interestingly, hCG and LH are both known scientifically as glycoproteins, which simply means that these hormones are made up of a protein with a sugar attached to it. Of even greater interest for this discussion, is the fact that the protein parts of hCG and LH look very similar. So similar, in fact, a standard ovulation test (OPK) is unable to distinguish between LH and hCG in your urine. Therefore, if you have enough of either of the two hormones (LH or hCG) in your urine at the time you test using an OPK, you will get a positive result on the OPK.
In theory, therefore, a positive result on an ovulation test taken after you have missed a period could definitely indicate that you are pregnant. But, while it might be tempting to use your extra ovulation test as a pregnancy test, most OPKs are not as sensitive as an early detection pregnancy test, which means that you will run the risk of getting a false negative...so, even if you are pregnant, your OPK will not be sensitive enough to detect the small amounts of hCG that are present in your urine in the first few days after conception. If you suspect that you have conceived, the quickest, most accurate way to confirm pregnancy is to use an early detection pregnancy test.
Why are they so mean!?
We're not mean. Really. We swear. We're protective with guarded hearts.
There have bee a few events lately that have lead to deleting of posts, rude things being said to other posters and a lot of hurt feelings in general.
That's why this blog is here. That is why this exists, to keep feelings from being hurt and joy and happiness to remain on the board.
First off, please remember the description of the board:
What does that mean exactly? That means that if you think you're pregnant, you're pregnant but not hopeful (unconfirmed) or are wanting to know how quickly someone got pregnant, or anything along any of those lines, Pregnant After A Loss is for you.
On Trying To Conceive After A Loss no one is pregnant, everyone wants to be and everyone has suffered a loss. There are some who are trying to not get pregnant for a while due to varying factors, but they know they will start to try again. They are on the board as well.
Everyone is there for one reason. Support.
Support must be given to be gotten. Make an introduction, get to know a few others, join in the random check-ins or book club. Please, please please, remember to make an intro, remember to keep pregnancies on Pregnant After A Loss and remember to be supportive.
Miscarriage/Pregnancy Loss Board
Trying To Conceive After A Loss Board
Pregnant After A Loss Board
There have bee a few events lately that have lead to deleting of posts, rude things being said to other posters and a lot of hurt feelings in general.
That's why this blog is here. That is why this exists, to keep feelings from being hurt and joy and happiness to remain on the board.
First off, please remember the description of the board:
If you have suffered a loss, you can also visit our Pregnancy Loss board. If you are pregnant after a loss, please visit Pregnant After a Loss.
What does that mean exactly? That means that if you think you're pregnant, you're pregnant but not hopeful (unconfirmed) or are wanting to know how quickly someone got pregnant, or anything along any of those lines, Pregnant After A Loss is for you.
On Trying To Conceive After A Loss no one is pregnant, everyone wants to be and everyone has suffered a loss. There are some who are trying to not get pregnant for a while due to varying factors, but they know they will start to try again. They are on the board as well.
Everyone is there for one reason. Support.
Support must be given to be gotten. Make an introduction, get to know a few others, join in the random check-ins or book club. Please, please please, remember to make an intro, remember to keep pregnancies on Pregnant After A Loss and remember to be supportive.
Miscarriage/Pregnancy Loss Board
Trying To Conceive After A Loss Board
Pregnant After A Loss Board
Stock up for Memorial Day
Early-Pregnancy-Tests.com is putting on an early Memorial Day sale!
What's on Sale?
Accupressure for Fertility DVD:
Harness the ancient healing power of acupressure to improve your chances of conceiving! Acupressure involves applying pressure to specific points on your body to improve blood flow to the reproductive organs and foster the body's vital life force (also known as "chi"). This program is specifically designed to enhance reproductive health in both men and women who are trying-to-conceive!
Use coupon code: pippa
FertilAid for Women: Optimize your chances of conceiving with FertilAid for Women – the doctor-designed supplement that provides complete vitamin supplementation while working to restore hormonal balance and promote reproductive wellness.
Order your supply now and save 10% off the regular price – and receive free same-day shipping!
Use coupon code: pippa
FertileCM:
FertileCM is a natural supplement designed to promote the production of fertile-quality cervical mucus – a key component in the trying-to-conceive equation. FertileCM also contains ingredients shown to help strengthen the uterine lining for implantation of the egg, and may also provide a "bump" in libido... ooh la la!
Order today and save 10% off the regular price – and receive free same-day shipping!
Use coupon code: pippa
Pregnancy and Ovulation Tests:
Save 10% off our flagship pregnancy tests, ovulation tests, and even our convenient conception combo packs!
Use coupon code: pippa
What's on Sale?
Accupressure for Fertility DVD:
Harness the ancient healing power of acupressure to improve your chances of conceiving! Acupressure involves applying pressure to specific points on your body to improve blood flow to the reproductive organs and foster the body's vital life force (also known as "chi"). This program is specifically designed to enhance reproductive health in both men and women who are trying-to-conceive!
Use coupon code: pippa
FertilAid for Women: Optimize your chances of conceiving with FertilAid for Women – the doctor-designed supplement that provides complete vitamin supplementation while working to restore hormonal balance and promote reproductive wellness.
Order your supply now and save 10% off the regular price – and receive free same-day shipping!
Use coupon code: pippa
FertileCM:
FertileCM is a natural supplement designed to promote the production of fertile-quality cervical mucus – a key component in the trying-to-conceive equation. FertileCM also contains ingredients shown to help strengthen the uterine lining for implantation of the egg, and may also provide a "bump" in libido... ooh la la!
Order today and save 10% off the regular price – and receive free same-day shipping!
Use coupon code: pippa
Pregnancy and Ovulation Tests:
Save 10% off our flagship pregnancy tests, ovulation tests, and even our convenient conception combo packs!
Use coupon code: pippa
When is it too much or too little?
Facing my own questions has raised some more. When is a period too heavy or too light? When is it too long or too short? Should I always have clots? What's a 'normal' cycle?
Some of you may know, I've been wondering why my periods randomly went from 4-5 days down to 1 and 1.5 days. Not only the length shortened, but I also went from heavy to very light. That started in November of 10. Now, it's started getting heavier and more painful, but has only lengthened to 2 days. So I wonder, is that too short?
Short Periods
From this Feb '10 publication, my answer would be yes. An article reviewed by Dr Pat Bass states " anywhere from three to seven days of bleeding is considered normal, and each full menstrual cycle can last anywhere from 21 to 35 days. Three days of bleeding, which may seem short, is still considered normal as long as you’re menstruating regularly." So, from this short quote, that would mean as long as your periods are regular, that's okay. But, that first part stating "3 days may seem short" leaves me wondering.
As I read in Taking Charge of Your Fertility, the time span between periods allows your endometrial lining to thicken. This is what allows for a healthy implantation. If there is no implantation, that lining comes of and is shown by the thickness and length of your period. Another published article, April '11, offers some insight; "Scanty blood flow however may also occur because ovulation is irregular at this time and the endometrial lining fails to develop normally."
So does that mean my lining is too thin? What if you have a long and heavy period? Can lining actually be too tick?
Long Periods
From the same April article, insight to long periods is also offered.
For those with long or heavy periods every moth that has become 'normal' for their body, there is a website and medication dedicated to lightening and shortening your periods called LightenMyPeriod.com
The Long and Short Of It
It seems no matter the information you find, they all say the same thing, if it's not 'normal' for you, call your doctor after two cycles. There are a variety of factors that could cause a long or short, heavy or light period. It could be thin or thick lining, clotting disorders, pregnancy, an unknown pregnancy loss, uterine abnormalities or hormone imbalances.
What if it's all been ruled out? Work on charting or using OPK's to help confirm ovulation in order to achieve pregnancy (or avoid). If ovulation is not detected or confirmed, consider discussing a month or two on birth control with your doctor. This may help balance hormones and get your body doing what it needs to, correctly.
REMEMBER: If you fill one pad or tampon per hour for 3 hours, call your OB, Dr, or go to the ER for too much blood loss.
Article to consider: MedlinePlus - April '09
Some of you may know, I've been wondering why my periods randomly went from 4-5 days down to 1 and 1.5 days. Not only the length shortened, but I also went from heavy to very light. That started in November of 10. Now, it's started getting heavier and more painful, but has only lengthened to 2 days. So I wonder, is that too short?
Short Periods
From this Feb '10 publication, my answer would be yes. An article reviewed by Dr Pat Bass states " anywhere from three to seven days of bleeding is considered normal, and each full menstrual cycle can last anywhere from 21 to 35 days. Three days of bleeding, which may seem short, is still considered normal as long as you’re menstruating regularly." So, from this short quote, that would mean as long as your periods are regular, that's okay. But, that first part stating "3 days may seem short" leaves me wondering.
As I read in Taking Charge of Your Fertility, the time span between periods allows your endometrial lining to thicken. This is what allows for a healthy implantation. If there is no implantation, that lining comes of and is shown by the thickness and length of your period. Another published article, April '11, offers some insight; "Scanty blood flow however may also occur because ovulation is irregular at this time and the endometrial lining fails to develop normally."
So does that mean my lining is too thin? What if you have a long and heavy period? Can lining actually be too tick?
Long Periods
From the same April article, insight to long periods is also offered.
A regular period typically lasts five days, but it is completely normal to menstruate for anywhere between three and seven days. More than a week therefore becomes abnormally long and could be due to changes in hormone levels, blood clotting or even uterus disorders.
For those with long or heavy periods every moth that has become 'normal' for their body, there is a website and medication dedicated to lightening and shortening your periods called LightenMyPeriod.com
The Long and Short Of It
It seems no matter the information you find, they all say the same thing, if it's not 'normal' for you, call your doctor after two cycles. There are a variety of factors that could cause a long or short, heavy or light period. It could be thin or thick lining, clotting disorders, pregnancy, an unknown pregnancy loss, uterine abnormalities or hormone imbalances.
What if it's all been ruled out? Work on charting or using OPK's to help confirm ovulation in order to achieve pregnancy (or avoid). If ovulation is not detected or confirmed, consider discussing a month or two on birth control with your doctor. This may help balance hormones and get your body doing what it needs to, correctly.
REMEMBER: If you fill one pad or tampon per hour for 3 hours, call your OB, Dr, or go to the ER for too much blood loss.
Article to consider: MedlinePlus - April '09
International Babylost Mothers Day
Today is Mothers Day for all those who's little ones cannot be held in arms, but rather in hearts.
http://internationalbabylostmothersday.blogspot.com/
Please share your love and support.
Feel free to grab either of the beautiful buttons provided by internationalbabylostmothersday.blogspot.com


http://internationalbabylostmothersday.blogspot.com/
Please share your love and support.
Feel free to grab either of the beautiful buttons provided by internationalbabylostmothersday.blogspot.com
Clomid
There is so much information you can find. You can hear many things from different doctors, find different websites contradicting each other and new studies always coming out make comfort hard to find.
Instead of doing research I decided it would be helpful to have input from those who we see every day who know what you'll go through, because they are.
Jkfranklin
BzeetyD
Carolee
Flagirl
A special thank you to all who offered advice and experience, it's very appreciated. If you have any questions that you'd like to ask these ladies or anyone else who might be going through what you are, please feel free to ask below or on the TTCAL board
Instead of doing research I decided it would be helpful to have input from those who we see every day who know what you'll go through, because they are.
Jkfranklin
After 15 cycles, I used clomid to get pg with my DS. I had no side effects at all. I had a base line vaginal u/s between CD1-3 and then took the clomid for 5 days (I want to say it was starting CD 5?) and then had another vaginal u/s to check my follies. They called me that day and told me to DB on Sunday morning and Monday morning (I believe I had the 2nd u/s on a Thursday or Friday). They guessed when I would O by the size. And about 2 weeks later I got my BFP.
BzeetyD
For the past 2 cycles TTC, started taking 50mg of Clomid days 3-7. Both times I experienced some significant bloating and some noticeable discomfort in my ovaries. The first cycle was the worst for these effects, the 2nd cycle wasn't as bad.
On CD12 or 13 (depending on when I thought I would O according to the opks I used) I got a follicle scan/ultrasound. The first cycle I had 2 good sized follies that our doc thought would go at the same time and 2 smaller follies that she thought would likely not rupture. The second cycle I had 1 great follicle and another decent sized one. She thought this time only one would go.
We were advised to BD every other day being sure to BD on the night of O - which both times for me was predicted as the same day I had my follicle scan.
We got PG on our 2nd cycle of Clomid (I was also taking Prometrium for the 2nd cycle). I got a positive test on 12dpo (10 and 11 dpo were negative).
When we're TTC again, we'll try the same dosage of 50mg. And of course we're hoping for a sticky healthy baby.
Carolee
I've taken Clomid for 7 cycles and am probably going to be starting my 8th tomorrow unless my RE changes meds on me.
I O on my own, but I am taking Clomid to increase my progesterone levels post-ovulation. I started at 50 mg, but when I started seeing my RE, he had me take 100 mg after telling me he never puts patients on 50 mg. I actually took it unmonitored for 4 cycles with my OB, but insisted on monitoring after that. Then my OB referred me to my RE. I discovered that many OBs hand Clomid out like candy and being monitored is really important because that way you know how you are responding (how many eggs you're producing and if your lining is decent). I have always taken Clomid on days 5-9 of my cycle. The only side effects I get are hot flashes and insomnia. The hot flashes last for the majority of my cycle, but the insomnia is really only when I'm taking the pills. I take it at night, and I have heard that can minimize side effects, which might be why I don't have that many.
Flagirl
I took Clomid for two cycles and got a BFP. Like others have said, I had to get an u/s between cd1-5. I started taking it cd 6-10. I get really bad cramps during O...(I did before Clomid, but I think its makes them worse) And other than that I didn't have any other side effects. This is my first cycle after my loss and I'm back on it!
A special thank you to all who offered advice and experience, it's very appreciated. If you have any questions that you'd like to ask these ladies or anyone else who might be going through what you are, please feel free to ask below or on the TTCAL board
Fertility Friend (FF) vs Taking Charge of Your Fertility (TCOYF)
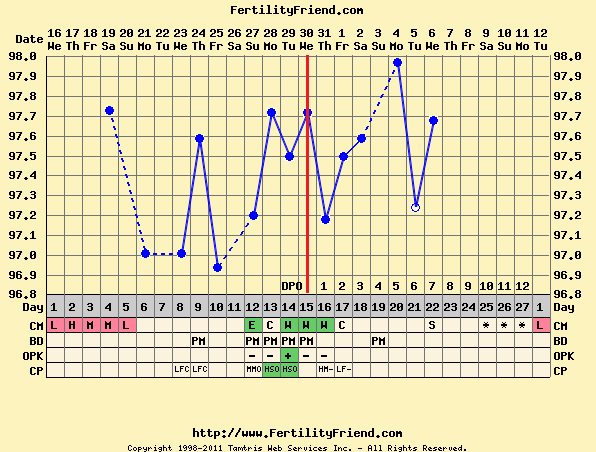
These are two great online resources for predicting and confirming ovulation and helping to determine your best chances of getting pregnant.
Both have the same base, you can chart your temperatures medications, cervical fluids, symptoms and your period (length and flow strength).
Each one is different in their own way and you have to look at and experience both before making your final decision.
Here are some threads on other boards about FF vs TCOYF on BabyCenter, WhatToExpect.com and even on TCYOF.com.
Personally, I have read TCOYF but I use FF. As of now, I do not take my temperature, use OPK's or check my cervical position, so it's very basic for me. I follow my days, my cervical fluids and sometimes my "symptoms".
Fertility Friend:

Taking Charge of Your Fertility:

Both sites are very user friendly, have forums and great tutorials. FF provides classes to get you started with charting and TCOYF has the book that is available for purchase. Whether you want to do a lot, like those pictured above, or a little, like me, there's a right match for you.
Have you looked at both? Which one is your favorite and why?
Both have the same base, you can chart your temperatures medications, cervical fluids, symptoms and your period (length and flow strength).
Each one is different in their own way and you have to look at and experience both before making your final decision.
Here are some threads on other boards about FF vs TCOYF on BabyCenter, WhatToExpect.com and even on TCYOF.com.
Personally, I have read TCOYF but I use FF. As of now, I do not take my temperature, use OPK's or check my cervical position, so it's very basic for me. I follow my days, my cervical fluids and sometimes my "symptoms".
Fertility Friend:
Taking Charge of Your Fertility:

Both sites are very user friendly, have forums and great tutorials. FF provides classes to get you started with charting and TCOYF has the book that is available for purchase. Whether you want to do a lot, like those pictured above, or a little, like me, there's a right match for you.
Have you looked at both? Which one is your favorite and why?
Mix Up The Meal results!!
It's time to show off (or tell off) what it was you made with this weeks ingredient: PEARS!
The recipe I chose was Grilled King Salmon with Pear Butter Sauce
I must say, it didn't turn out looking like the picture, but it tasted very delicious!
Ingredients
3 tablespoons olive oil
4 (6-ounce) Alaskan salmon fillets
Salt and freshly ground white pepper
Pear-butter sauce:
2 firm-ripe pears, such as Bartlett, peeled, cored and diced
2 tablespoons packed light brown sugar
1/2 cup hard cider
1/2 cup heavy cream
2 sticks (1/2 pound) cold unsalted butter, cut into pieces
Salt and freshly ground white pepper
Herb Roasted Fingerling Potatoes, recipe follows
Directions
Preheat grill to medium-high and coat with oil.
Season both sides of each salmon fillet with salt and pepper and place on the grill. Grill until the center is still slightly pink, 6 to 8 minutes total, rotating fish 90 degrees halfway during cooking on each side to obtain hash marks. Remove from the grill.
Meanwhile, make the pear butter sauce: In a medium saucepan, combine the diced pears, sugar, and hard cider. Cook over medium-high heat until the pears are translucent, about 5 minutes. Add the cream and cook until reduced by half, about 6 minutes. Add the butter several pieces at a time, whisking constantly to blend, and removing from the heat periodically to prevent the sauce from breaking. Add 1/4 teaspoon salt and 1/8 teaspoon white pepper and whisk to blend. Remove from the heat and cover to keep warm until ready to serve, stirring occasionally. (Do not allow sauce to boil or it will separate.)
Place the salmon on the plate with the roasted potatoes, drizzle the pear butter over the salmon and serve immediately.
What did you make!? Show it off below or in this thread
The recipe I chose was Grilled King Salmon with Pear Butter Sauce
I must say, it didn't turn out looking like the picture, but it tasted very delicious!
Ingredients
3 tablespoons olive oil
4 (6-ounce) Alaskan salmon fillets
Salt and freshly ground white pepper
Pear-butter sauce:
2 firm-ripe pears, such as Bartlett, peeled, cored and diced
2 tablespoons packed light brown sugar
1/2 cup hard cider
1/2 cup heavy cream
2 sticks (1/2 pound) cold unsalted butter, cut into pieces
Salt and freshly ground white pepper
Herb Roasted Fingerling Potatoes, recipe follows
Directions
Preheat grill to medium-high and coat with oil.
Season both sides of each salmon fillet with salt and pepper and place on the grill. Grill until the center is still slightly pink, 6 to 8 minutes total, rotating fish 90 degrees halfway during cooking on each side to obtain hash marks. Remove from the grill.
Meanwhile, make the pear butter sauce: In a medium saucepan, combine the diced pears, sugar, and hard cider. Cook over medium-high heat until the pears are translucent, about 5 minutes. Add the cream and cook until reduced by half, about 6 minutes. Add the butter several pieces at a time, whisking constantly to blend, and removing from the heat periodically to prevent the sauce from breaking. Add 1/4 teaspoon salt and 1/8 teaspoon white pepper and whisk to blend. Remove from the heat and cover to keep warm until ready to serve, stirring occasionally. (Do not allow sauce to boil or it will separate.)
Place the salmon on the plate with the roasted potatoes, drizzle the pear butter over the salmon and serve immediately.
What did you make!? Show it off below or in this thread
What is this stuff? Cervical Fluids
"Typical" Cervical Fluid Pattern
While your cervical fluid pattern may vary from cycle to cycle and it may vary from woman to woman, a typical cervical fluid pattern looks like this:
Immediately following menstruation there is usually a dry vaginal sensation and there is little or no cervical fluid.
After a few days of dryness, there is normally a cervical fluid that is best described as "sticky" or "pasty" but not wet. While this kind of cervical fluid is not conducive to sperm survival these days may be considered as "possibly fertile" if found before ovulation.
Following these "sticky" days, most women generally notice a cervical fluid that is best described as "creamy". This fluid may be white, yellow or beige in color and has the look and feel of lotion or cream. At this point the vagina may feel wet and this indicates possible increased fertility.
The most fertile cervical fluid now follows. This most fertile fluid looks and feels like raw egg white. It is slippery and may be stretched several inches between your fingers. It is usually clear and may be very watery. The vagina feels wet and lubricated. These days are considered most fertile. This is the fluid that is the most friendly and receptive to sperm. It looks a lot like semen and, like semen, can act as a transport for sperm.
After ovulation, fertile fluid dries up very quickly and the vagina remains more or less dry until the next cycle. Some women may notice small amounts of fertile-looking fluid after ovulation as the corpus luteum produces small amounts of estrogen, but you are not at all fertile after ovulation has been confirmed.
Cervical Fluid and Their Meaning
Dry - Probably Not Fertile
Sticky - Probably Not Fertile
Creamy - Possibly Fertile
Watery - Fertile
Egg white - Most Fertile
How can I tell the difference between fertile cervical fluid and semen?
If you find that you have more watery or eggwhite days than you would expect and that these often follow days or nights that you had intercourse, then you may be mistaking seminal and cervical fluid. They have similar properties because they share the same function: transporting and nourishing sperm. You will find, however, that fertile cervical fluid (eggwhite) is more clear and stretchy and shiny. It will stretch a couple of inches without breaking. Semen may be more whitish and is more likely to break when pulled.
If you are in doubt and it is near your fertile time, always record eggwhite cervical fluid, even if it may be obscured by seminal fluid. This way, you will not miss a potentially fertile time. Emitting semen immediately after intercourse by doing kegel exercises (which is sometimes recommended for people who are charting to avoid pregnancy so that cervical fluid is not obscured) is not recommended when you are trying to conceive. While most sperm reach their destination within your reproductive tract quite quickly after intercourse, you don't want to sacrifice your chances of conception to have a perfect chart.
Taken directly from Fertility Friend
While your cervical fluid pattern may vary from cycle to cycle and it may vary from woman to woman, a typical cervical fluid pattern looks like this:
Immediately following menstruation there is usually a dry vaginal sensation and there is little or no cervical fluid.
After a few days of dryness, there is normally a cervical fluid that is best described as "sticky" or "pasty" but not wet. While this kind of cervical fluid is not conducive to sperm survival these days may be considered as "possibly fertile" if found before ovulation.
Following these "sticky" days, most women generally notice a cervical fluid that is best described as "creamy". This fluid may be white, yellow or beige in color and has the look and feel of lotion or cream. At this point the vagina may feel wet and this indicates possible increased fertility.
The most fertile cervical fluid now follows. This most fertile fluid looks and feels like raw egg white. It is slippery and may be stretched several inches between your fingers. It is usually clear and may be very watery. The vagina feels wet and lubricated. These days are considered most fertile. This is the fluid that is the most friendly and receptive to sperm. It looks a lot like semen and, like semen, can act as a transport for sperm.
After ovulation, fertile fluid dries up very quickly and the vagina remains more or less dry until the next cycle. Some women may notice small amounts of fertile-looking fluid after ovulation as the corpus luteum produces small amounts of estrogen, but you are not at all fertile after ovulation has been confirmed.
Cervical Fluid and Their Meaning
Dry - Probably Not Fertile
Sticky - Probably Not Fertile
Creamy - Possibly Fertile
Watery - Fertile
Egg white - Most Fertile
How can I tell the difference between fertile cervical fluid and semen?
If you find that you have more watery or eggwhite days than you would expect and that these often follow days or nights that you had intercourse, then you may be mistaking seminal and cervical fluid. They have similar properties because they share the same function: transporting and nourishing sperm. You will find, however, that fertile cervical fluid (eggwhite) is more clear and stretchy and shiny. It will stretch a couple of inches without breaking. Semen may be more whitish and is more likely to break when pulled.
If you are in doubt and it is near your fertile time, always record eggwhite cervical fluid, even if it may be obscured by seminal fluid. This way, you will not miss a potentially fertile time. Emitting semen immediately after intercourse by doing kegel exercises (which is sometimes recommended for people who are charting to avoid pregnancy so that cervical fluid is not obscured) is not recommended when you are trying to conceive. While most sperm reach their destination within your reproductive tract quite quickly after intercourse, you don't want to sacrifice your chances of conception to have a perfect chart.
Taken directly from Fertility Friend
OPK's- What you need to know and how you need to know it
I am going to preface by saying this: You may get one surge that will lead to ovulation. You may get a surge that will not lead to ovulation. You may get multiple surges leading to no ovulation. You may get near positives and never get an actual positive. You may have PCOS or other hormonal complications that will never allow you to surge or ovulate. You may have constant lines and never surge.
There are many variables and many ways that ovulation tests can be viewed or read.
************************************************************
If you read the post about home pregnancy test varieties, this one will blow it away. Pregnancy tests are simple. You can test with blood, a stream of urine or urine in a cup. With ovulation tests you can test with a stream of urine, urine in a cup, taking your temperature every morning at the same time, using a watch during certain time periods and also through blood tests or ultrasounds.
This post will only talk about a few. Midstream and cup collection will be the two biggest. There will be a small bit about taking temperature and using the watch or monitor, so bear with me.
Midstream tests
There are variety of companies who create midstream OPK’s. ClearBlue, Answer and those from Early-Pregnancy-Tests.com are some of the more popular. These tests look like the home pregnancy tests, so make sure you have them separated so you can identify them properly.
With these tests you will get a smiley face for the digitals and a line for the regular version. For your lines, you want the test line to be AS DARK OR DARKER THAN the control line. Remember, you may always have a line there, but it’s lighter when you do not have a surge.
If you use the ClearBlue digital OPK, DO NOT open it and analyze the lines inside. They are often lighter than the control and will confuse you. Trust your smiley face or empty circle to tell you the truth.


Dipping tests
These are often referred to as the “internet cheapies” or Wondfo's. They’re small strips you dip into a cup of collected urine. These are my personal favorite. They’re cheap, easy to transport and easy to read. You must follow the instructions properly to insure you get the right answer. Early-pregnancy-tests.com and Amazon have great deals on them.
The same goes with these as with the midstream. The test line must be AS DARK OR DARKER THAN the control line. If your lines smear or there is no control, test again. That’s what’s great about the dipping ones. You don’t have to pee again, just use the same collection.

Temping
Full fledged charters will also use a basal body thermometer to help determine ovulation. Please note: This will NOT predict ovulation, but it will help confirm what an OPK will predict.
With temping, you take your tempature every morning at the same time after 3 or more hours of sleep. There are many rules when it comes to temping the proper way to get the proper answers. Please ask questions and read Taking Charge Of Your Fertility. It’s a FANTASTIC book with questions you’ll have and their answers, scenarios played out and charts to help get you started. Also check out FertilityFriend.com. It’s an online version of charting that has “classes” to teach you.
Using a watch or monitor
No, I don’t mean a regular watch, I mean the OvWatch. This watch requires you to follow specific instructions when wearing it, how to read it properly and sensors to be used.

The monitor I’m referring to is the ClearBlue Easy Fertility Monitor. It’s expensive, requires sensors daily and can be difficult to read if you don’t follow the instructions. I have heard great reviews and outcomes. You can also often find the monitor and/or sensors on Ebay or Amazon for decent prices.

There are many ways to help find out the right times to time sex to achieve pregnancy or to avoid it. These are only a few ways. Never be afraid to ask questions. I HIGHLY recommend reading the book, it will answer so many questions you never knew you had. You can find some on Ebay, Amazon, Barnes&Noble and many more places.
What is it you like to pee on for that perfect timing? Join us in this thread or comment below to share your favorite, or the one you refuse to use!
There are many variables and many ways that ovulation tests can be viewed or read.
************************************************************
If you read the post about home pregnancy test varieties, this one will blow it away. Pregnancy tests are simple. You can test with blood, a stream of urine or urine in a cup. With ovulation tests you can test with a stream of urine, urine in a cup, taking your temperature every morning at the same time, using a watch during certain time periods and also through blood tests or ultrasounds.
This post will only talk about a few. Midstream and cup collection will be the two biggest. There will be a small bit about taking temperature and using the watch or monitor, so bear with me.
Midstream tests
There are variety of companies who create midstream OPK’s. ClearBlue, Answer and those from Early-Pregnancy-Tests.com are some of the more popular. These tests look like the home pregnancy tests, so make sure you have them separated so you can identify them properly.
With these tests you will get a smiley face for the digitals and a line for the regular version. For your lines, you want the test line to be AS DARK OR DARKER THAN the control line. Remember, you may always have a line there, but it’s lighter when you do not have a surge.
If you use the ClearBlue digital OPK, DO NOT open it and analyze the lines inside. They are often lighter than the control and will confuse you. Trust your smiley face or empty circle to tell you the truth.


Dipping tests
These are often referred to as the “internet cheapies” or Wondfo's. They’re small strips you dip into a cup of collected urine. These are my personal favorite. They’re cheap, easy to transport and easy to read. You must follow the instructions properly to insure you get the right answer. Early-pregnancy-tests.com and Amazon have great deals on them.
The same goes with these as with the midstream. The test line must be AS DARK OR DARKER THAN the control line. If your lines smear or there is no control, test again. That’s what’s great about the dipping ones. You don’t have to pee again, just use the same collection.

Temping
Full fledged charters will also use a basal body thermometer to help determine ovulation. Please note: This will NOT predict ovulation, but it will help confirm what an OPK will predict.
With temping, you take your tempature every morning at the same time after 3 or more hours of sleep. There are many rules when it comes to temping the proper way to get the proper answers. Please ask questions and read Taking Charge Of Your Fertility. It’s a FANTASTIC book with questions you’ll have and their answers, scenarios played out and charts to help get you started. Also check out FertilityFriend.com. It’s an online version of charting that has “classes” to teach you.
Using a watch or monitor
No, I don’t mean a regular watch, I mean the OvWatch. This watch requires you to follow specific instructions when wearing it, how to read it properly and sensors to be used.

The monitor I’m referring to is the ClearBlue Easy Fertility Monitor. It’s expensive, requires sensors daily and can be difficult to read if you don’t follow the instructions. I have heard great reviews and outcomes. You can also often find the monitor and/or sensors on Ebay or Amazon for decent prices.

There are many ways to help find out the right times to time sex to achieve pregnancy or to avoid it. These are only a few ways. Never be afraid to ask questions. I HIGHLY recommend reading the book, it will answer so many questions you never knew you had. You can find some on Ebay, Amazon, Barnes&Noble and many more places.
What is it you like to pee on for that perfect timing? Join us in this thread or comment below to share your favorite, or the one you refuse to use!
Videos to love
This one was found by Jen629, it's Hold by Michael Buble
This one was heard on the radio by me and I love it.
This one was heard on the radio by me and I love it.
Playing Catch up!
First- Lets do the Mix Up The Meal Recipe! I think we can come up with some fantastic meals with.........PEARS!

No, I'm not asking you to cook a gourmet meal with 5 courses and be all decked out, just find a good fun way to use an ingredient, be it a lot or a little. Each week, there will be a new ingredient. Every Friday, we'll go over what was created and how it tasted and you can even throw in a picture if you'd like!
There are different flavors and makes of this great product, so do some browsing on Google, Recipes.com, allrecipes.com or foodnetwork.com. Either way, you'll be good to go! Desserts are welcome as well! Just remember, get creative!
Second- Later today, the OPK comparison post will be coming out. There's a TON of information to put together, thats part of why it's taken so long to come out.
Finally- Don't forget about the Mothers Day Gift Exchange. Names will be drawn on the 9th. No more entries after the 8th!
Here is the link if you need it: TTCAL Mothers Day Gift Exchange

No, I'm not asking you to cook a gourmet meal with 5 courses and be all decked out, just find a good fun way to use an ingredient, be it a lot or a little. Each week, there will be a new ingredient. Every Friday, we'll go over what was created and how it tasted and you can even throw in a picture if you'd like!
There are different flavors and makes of this great product, so do some browsing on Google, Recipes.com, allrecipes.com or foodnetwork.com. Either way, you'll be good to go! Desserts are welcome as well! Just remember, get creative!
Second- Later today, the OPK comparison post will be coming out. There's a TON of information to put together, thats part of why it's taken so long to come out.
Finally- Don't forget about the Mothers Day Gift Exchange. Names will be drawn on the 9th. No more entries after the 8th!
Here is the link if you need it: TTCAL Mothers Day Gift Exchange
Mix Up The Meal results!!
What did you make with this weeks ingredient? APPLESAUCE!!
Share your recipe and/or photos if you'd like!
My recipe (Noah-bear)
Applesauce Cookies
Ingredients
1 cup(s) flour
1 teaspoon(s) cinnamon
1 teaspoon(s) baking soda
1/2 teaspoon(s) salt
1/2 cup(s) your favorite nuts
1 cup(s) quick oats (not instant oatmeal)
1 cup(s) raisins
1 cup(s) applesauce
2 eggs
1/2 cup(s) vegetable oil
1 teaspoon(s) vanilla extract
Directions
Preheat the oven to 375 degrees.
Mix the dry ingredients in the largest bowl. Mix the wet ingredients in the other bowl. Add the dry mixture to the wet mixture. Blend them well.
Spoon the dough for these drop cookies onto the greased cookie sheets.
Bake the dough for 8 to 10 minutes.
Allow the cookies to cool before eating them.
Share your recipe and/or photos if you'd like!
My recipe (Noah-bear)
Applesauce Cookies
Ingredients
1 cup(s) flour
1 teaspoon(s) cinnamon
1 teaspoon(s) baking soda
1/2 teaspoon(s) salt
1/2 cup(s) your favorite nuts
1 cup(s) quick oats (not instant oatmeal)
1 cup(s) raisins
1 cup(s) applesauce
2 eggs
1/2 cup(s) vegetable oil
1 teaspoon(s) vanilla extract
Directions
Preheat the oven to 375 degrees.
Mix the dry ingredients in the largest bowl. Mix the wet ingredients in the other bowl. Add the dry mixture to the wet mixture. Blend them well.
Spoon the dough for these drop cookies onto the greased cookie sheets.
Bake the dough for 8 to 10 minutes.
Allow the cookies to cool before eating them.
A different child
This poem was shared on the Pregnant After A Loss board and it was requested it be shared on this blog. It's powerful.
A Different Child
A different child, people notice
There's a special glow around you.
You grow surrounded by love
Never doubting you are wanted;
Only look at the pride and joy
In your mother and father's eyes.
And if sometimes between the smiles
There's a trace of tears,
One day you'll understand.
You'll understand there was once another child.
A different child.
Who was in their hopes and dreams.
That child will never outgrow the baby clothes.
That child will never keep them up at night.
In fact, that child will never be any trouble at all...
Except sometimes, in a silent moment,
When mother and father miss so much
That different child.
May hope and love wrap you warmly
And may you learn the lesson forever:
How infinitely precious,
How infinitely fragile is this life on earth.
One day, as a young man or woman
You may see another mother's tears
Another father's silent grief
Then you, and you alone will understand
And offer the greatest comfort.
When all hope seems lost
you will tell them with great compassion:
"I know how you feel.
I'm only here because my parents tried again."
Author Unknown
A Different Child
A different child, people notice
There's a special glow around you.
You grow surrounded by love
Never doubting you are wanted;
Only look at the pride and joy
In your mother and father's eyes.
And if sometimes between the smiles
There's a trace of tears,
One day you'll understand.
You'll understand there was once another child.
A different child.
Who was in their hopes and dreams.
That child will never outgrow the baby clothes.
That child will never keep them up at night.
In fact, that child will never be any trouble at all...
Except sometimes, in a silent moment,
When mother and father miss so much
That different child.
May hope and love wrap you warmly
And may you learn the lesson forever:
How infinitely precious,
How infinitely fragile is this life on earth.
One day, as a young man or woman
You may see another mother's tears
Another father's silent grief
Then you, and you alone will understand
And offer the greatest comfort.
When all hope seems lost
you will tell them with great compassion:
"I know how you feel.
I'm only here because my parents tried again."
Author Unknown
I need to pee, but what on?
Going to the "family planning" section of the store can be a little overwhelming. You don't want to sacrifice results for a price and you don't want to get your heart broken by false positives
Between the blue dyes, pink dyes, smilies, words, and midstream or cup variations of a "pee stick", it's hard to choose the right one.
What should you look for in a HPT?
It's commonly known that blue dye tests are notorious for false positives. Pink dyes have been known to give good, early, reliable results. Digitals are more expensive and also have been said to have a harder time detecting a pregnancy early on.
Don't just look for the price tag, but don't think you have to buy the most expensive on the market. You can find good reliable tests, yes, even generic, for a price that wont hurt.
You can also choose between midstream tests or the kind where you pee in a cup and dip the test. The more popular is midstream, but you can purchase the dip tests online for quite a good price break. Check Amazon or Early-Pregnancy-Tests.com.
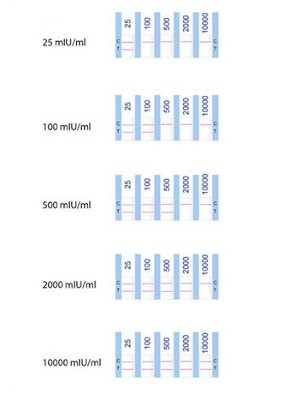
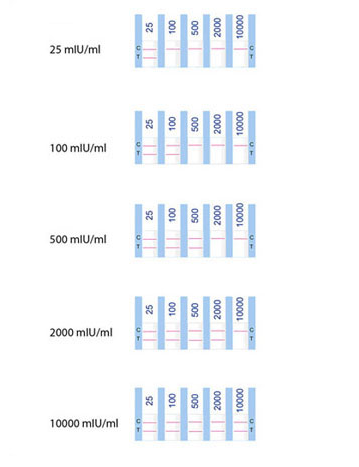
What makes them all different?
As your hCG increases with pregnancy, so do the chances of picking up the hormones on the test strip. Many brands can detect a pregnancy at different points and some are more sensitive than others.
Here's a wonderful chart from Early-Pregnancy-Tests.com

As you can see, the numbers can vary greatly. The higher the number, the harder it is to detect the hormones early on.
FMU, HPT, POAS, PIAC, what does it mean!?
There are many acronyms when it comes to this subject.
FMU= First Morning Urine. It's recommended to use your urine first thing in the morning because it's the most concentrated and will have the highest hormone level.
HPT= Home Pregnancy Test, both midstream and dip tests.
POAS= Pee On A Stick, commonly known as mid-stream tests. These are the ones with the plastic body and tip that is used to catch urine, also comes with a reading window.
PIAC= Pee In A Cup, these tests are for the ovulation tests and home pregnancy tests that you dip into a cup of collected urine. *NOTE you do not dip it in the toilet*
The dip tests are generally cheaper and you can buy in bulk fairly well, both Amazon and Early-Pregnancy-Tests.com will have great options.
Please check the side of this page --->
Note the chart stating the percentage chance of you getting a positive test at a specific number of DPO (Days Past Ovulation). Testing early will increase your chances for a negative, remember to be prepared for it being too early.
What's your favorite brand to pee on? Join our thread Here or comment below!
Between the blue dyes, pink dyes, smilies, words, and midstream or cup variations of a "pee stick", it's hard to choose the right one.
What should you look for in a HPT?
It's commonly known that blue dye tests are notorious for false positives. Pink dyes have been known to give good, early, reliable results. Digitals are more expensive and also have been said to have a harder time detecting a pregnancy early on.
Don't just look for the price tag, but don't think you have to buy the most expensive on the market. You can find good reliable tests, yes, even generic, for a price that wont hurt.
You can also choose between midstream tests or the kind where you pee in a cup and dip the test. The more popular is midstream, but you can purchase the dip tests online for quite a good price break. Check Amazon or Early-Pregnancy-Tests.com.
What makes them all different?
As your hCG increases with pregnancy, so do the chances of picking up the hormones on the test strip. Many brands can detect a pregnancy at different points and some are more sensitive than others.
Here's a wonderful chart from Early-Pregnancy-Tests.com

As you can see, the numbers can vary greatly. The higher the number, the harder it is to detect the hormones early on.
FMU, HPT, POAS, PIAC, what does it mean!?
There are many acronyms when it comes to this subject.
FMU= First Morning Urine. It's recommended to use your urine first thing in the morning because it's the most concentrated and will have the highest hormone level.
HPT= Home Pregnancy Test, both midstream and dip tests.
POAS= Pee On A Stick, commonly known as mid-stream tests. These are the ones with the plastic body and tip that is used to catch urine, also comes with a reading window.
PIAC= Pee In A Cup, these tests are for the ovulation tests and home pregnancy tests that you dip into a cup of collected urine. *NOTE you do not dip it in the toilet*
The dip tests are generally cheaper and you can buy in bulk fairly well, both Amazon and Early-Pregnancy-Tests.com will have great options.
Please check the side of this page --->
Note the chart stating the percentage chance of you getting a positive test at a specific number of DPO (Days Past Ovulation). Testing early will increase your chances for a negative, remember to be prepared for it being too early.
What's your favorite brand to pee on? Join our thread Here or comment below!
Mothers [of Angels] Day - Elfster Gift Exchange
Elfster is a secret santa gift exchange. We've done them in the past here on TTCAL, and it becomes a lot of fun. So why not do one for Mothers Day!? If you'd like to join, please follow the directions below.
Here's the details for those new to Elfster:
Here's the details for those new to Elfster:
Sign-up before Friday, April 8th (I'll post multiple reminders in the evening, too).
To sign-up click on the link below and follow the instructions. When you sign up be sure to include somewhere your bump screen name to help your elfster identify you. http://www.elfster.com/exchange/view/5111011/e0677f/
After the sign-up deadline, Elfster will randomly assign you an elfster buddy and notify you via email of their name and a mailing address.
You will be able ask (anonymously) your person any questions that may help in selecting the right gift.
As for the gift - I put a $20 suggested limit on this one but am open if you guys want to change it. I was thinking a card, Hallmark-ish plaque, bookmark, etc... just something that recognizes and honors them as mothers.
And most importantly - remember to get the gift in the mail so it arrives before Mother's Day - May 8th.
We'll set our reveal date for Monday, May 9th!
Time to Mix Up The Meals!
It's Monday, so most people are working on grocery lists, menu's for the week and looking up recipes.
So, lets add a little fun to the week and get creative!
No, I'm not asking you to cook a gourmet meal with 5 courses and be all decked out, just find a good fun way to use an ingredient, be it a lot or a little. Each week, there will be a new ingredient. Every Friday, we'll go over what was created and how it tasted and you can even throw in a picture if you'd like!
So....this weeks ingredient ::drumroll::

APPLESAUCE!!
There are so many ways to use applesauce, so lets see what you've got. And no, you can't pour it in a bowl and top it with cinnamon ;-)
There are different flavors and makes of this great product, so do some browsing on Google, Recipes.com, allrecipes.com or foodnetwork.com. Either way, you'll be good to go! Desserts are welcome as well! Just remember, get creative!
So, lets add a little fun to the week and get creative!
No, I'm not asking you to cook a gourmet meal with 5 courses and be all decked out, just find a good fun way to use an ingredient, be it a lot or a little. Each week, there will be a new ingredient. Every Friday, we'll go over what was created and how it tasted and you can even throw in a picture if you'd like!
So....this weeks ingredient ::drumroll::

APPLESAUCE!!
There are so many ways to use applesauce, so lets see what you've got. And no, you can't pour it in a bowl and top it with cinnamon ;-)
There are different flavors and makes of this great product, so do some browsing on Google, Recipes.com, allrecipes.com or foodnetwork.com. Either way, you'll be good to go! Desserts are welcome as well! Just remember, get creative!
Polycystic Ovary Syndrome- PCOS
First off. What is PCOS?
Polycystic ovary syndrome is a condition in which there is an imbalance of a woman's female sex hormones. This hormone imbalance may cause changes in the menstrual cycle, skin changes, small cysts in the ovaries, trouble getting pregnant, and other problems.
PCOS is one of the most common causes of fertility issues in women, but it's rarely addressed publicly and can be, at times, hard to diagnose. Starting as young as 13 or 14 and ranging up to menopause, PCOS can affect any woman and with a variety of symptoms.
Symptoms of PCOS can be mild, moderate or severe. They can also be a 'coctail' of any that are listed below:
Changes in the menstrual cycle:
Absent periods, usually with a history of having one or more normal menstrual periods during puberty (secondary amenorrhea)
Irregular menstrual periods, which may be more or less frequent, and may range from very light to very heavy
Development of male sex characteristics (virilization):
Decreased breast size
Deepening of the voice
Enlargement of the clitoris
Increased body hair on the chest, abdomen, and face, as well as around the nipples (called hirsutism)
Thinning of the hair on the head, called male-pattern baldness
Other skin changes:
Acne that gets worse
Dark or thick skin markings and creases around the armpits, groin, neck, and breasts due to insulin sensitivity
Some women may only exhibit irregular periods or some women may have irregular periods, increased hair, insulin resistance, elevated testosterone, etc. all at once.
When you sit down with your Dr, OB or Endochronologist, and list out your symptoms, be they many or one, you may be given a round of testing. These tests will determine your insulin, how it's processed, your testosterone, estrogen and thyroid. There are other tests that may be run, but the previous listed are the most common. Other tests may include:
Once a diagnosis is confirmed, treatment may begin. As varying of the symptoms, so are the treatments. Some may only need a diet and weight modification. Others may need medications as well as diet and exercise adjustments. All will be an effort to balance hormones and increase ovulation regularity.
Medications include:
Birth control pills or progesterone
Metformin or Clomid
LH-releasing hormone (LHRH) analogs
Only you and your doctor can determine what the best course of action is. If you are ever uncomfortable with a diagnosis or treatment, seek a second opinion. Learning from others with the same experience can also be beneficial. There are two fantastic groups called SoulCysters and PCOSSupport that can help connect you with others, give you information and help guide you through this confusing time.
Never be afraid to ask a question or ask for help. PCOS can be confusing and scary at times. Follow directions and try to stick to a healthy diet and exercise routine.
Additional information:
Medical publication- http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001408/
WebMD Overview- http://women.webmd.com/tc/polycystic-ovary-syndrome-pcos-topic-overview
Medications- http://www.newsmax.com/FastFeatures/Polycystic-Ovary-Syndrome-drugs/2011/03/09/id/370670
Polycystic ovary syndrome is a condition in which there is an imbalance of a woman's female sex hormones. This hormone imbalance may cause changes in the menstrual cycle, skin changes, small cysts in the ovaries, trouble getting pregnant, and other problems.
PCOS is one of the most common causes of fertility issues in women, but it's rarely addressed publicly and can be, at times, hard to diagnose. Starting as young as 13 or 14 and ranging up to menopause, PCOS can affect any woman and with a variety of symptoms.
Symptoms of PCOS can be mild, moderate or severe. They can also be a 'coctail' of any that are listed below:
Changes in the menstrual cycle:
Absent periods, usually with a history of having one or more normal menstrual periods during puberty (secondary amenorrhea)
Irregular menstrual periods, which may be more or less frequent, and may range from very light to very heavy
Development of male sex characteristics (virilization):
Decreased breast size
Deepening of the voice
Enlargement of the clitoris
Increased body hair on the chest, abdomen, and face, as well as around the nipples (called hirsutism)
Thinning of the hair on the head, called male-pattern baldness
Other skin changes:
Acne that gets worse
Dark or thick skin markings and creases around the armpits, groin, neck, and breasts due to insulin sensitivity
Some women may only exhibit irregular periods or some women may have irregular periods, increased hair, insulin resistance, elevated testosterone, etc. all at once.
When you sit down with your Dr, OB or Endochronologist, and list out your symptoms, be they many or one, you may be given a round of testing. These tests will determine your insulin, how it's processed, your testosterone, estrogen and thyroid. There are other tests that may be run, but the previous listed are the most common. Other tests may include:
Estrogen levels
FSH levels
LH levels
17-ketosteroids
Lipid levels
Pregnancy test (serum HCG)
Prolactin levels
Vaginal ultrasound to look at the ovaries
Pelvic laparoscopy to look more closely at, and possibly biopsy the ovaries
Once a diagnosis is confirmed, treatment may begin. As varying of the symptoms, so are the treatments. Some may only need a diet and weight modification. Others may need medications as well as diet and exercise adjustments. All will be an effort to balance hormones and increase ovulation regularity.
Medications include:
Birth control pills or progesterone
Metformin or Clomid
LH-releasing hormone (LHRH) analogs
Only you and your doctor can determine what the best course of action is. If you are ever uncomfortable with a diagnosis or treatment, seek a second opinion. Learning from others with the same experience can also be beneficial. There are two fantastic groups called SoulCysters and PCOSSupport that can help connect you with others, give you information and help guide you through this confusing time.
Never be afraid to ask a question or ask for help. PCOS can be confusing and scary at times. Follow directions and try to stick to a healthy diet and exercise routine.
Additional information:
Medical publication- http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001408/
WebMD Overview- http://women.webmd.com/tc/polycystic-ovary-syndrome-pcos-topic-overview
Medications- http://www.newsmax.com/FastFeatures/Polycystic-Ovary-Syndrome-drugs/2011/03/09/id/370670
"Genes for Pre-Eclampsia Discovered"
BBC Article
Scientists say they have identified genetic errors that appear to increase a pregnant woman's chance of getting the potentially life-threatening condition called pre-eclampsia.
Around four in every 100 women develops this problem of high blood pressure and leaky kidneys during pregnancy.
Now researchers have found faulty DNA may be to blame in some cases, PLoS Medicine journal reports.
The discovery could lead to new ways to spot and treat those at risk, they say.
The US researchers from the Washington University School of Medicine in St. Louis analysed DNA from over 300 pregnant women.
Sixty of these were otherwise healthy women who were hospitalised because they developed severe pre-eclampsia.
The remaining 250 were women who were being monitored for other health complications. Forty of these also went on to develop pre-eclampsia.
DNA analysis revealed a few genetic errors shared by five of the 60 otherwise healthy women and seven of the 40 "higher-risk pregnancy" women who developed pre-eclampsia.
The genes on which the errors were identified (MCP factor I and factor H) play a role in regulating immune response and the researchers believe this could explain their possible link to pre-eclampsia.
Scientists have suspected that problems with the immune system provoke many cases of pre-eclampsia because women with lupus and certain other autoimmune diseases - like 250 of the women in the study - have an increased risk of the disorder.
The researchers now plan to study more pregnant women and other genes to further their understanding.
Professor Basky Thilaganathan, spokesman for the Royal College of Obstetricians and Gynaecologists, said: "This work shows an association.
"At best genes like these might identify 10-15% of pre-eclampsia, so it's relative importance may not be sensational. But it may allow us to study new treatments to prevent or delay the onset of pre-eclampsia and to know which women need closer surveillance."
He said that currently the only real way to halt the condition was to deliver the baby. This can be relatively risk free if the pregnancy is nearing its natural end anyway, but can be risky if the baby is premature.
Scientists say they have identified genetic errors that appear to increase a pregnant woman's chance of getting the potentially life-threatening condition called pre-eclampsia.
Around four in every 100 women develops this problem of high blood pressure and leaky kidneys during pregnancy.
Now researchers have found faulty DNA may be to blame in some cases, PLoS Medicine journal reports.
The discovery could lead to new ways to spot and treat those at risk, they say.
The US researchers from the Washington University School of Medicine in St. Louis analysed DNA from over 300 pregnant women.
Sixty of these were otherwise healthy women who were hospitalised because they developed severe pre-eclampsia.
The remaining 250 were women who were being monitored for other health complications. Forty of these also went on to develop pre-eclampsia.
DNA analysis revealed a few genetic errors shared by five of the 60 otherwise healthy women and seven of the 40 "higher-risk pregnancy" women who developed pre-eclampsia.
The genes on which the errors were identified (MCP factor I and factor H) play a role in regulating immune response and the researchers believe this could explain their possible link to pre-eclampsia.
Scientists have suspected that problems with the immune system provoke many cases of pre-eclampsia because women with lupus and certain other autoimmune diseases - like 250 of the women in the study - have an increased risk of the disorder.
The researchers now plan to study more pregnant women and other genes to further their understanding.
Professor Basky Thilaganathan, spokesman for the Royal College of Obstetricians and Gynaecologists, said: "This work shows an association.
"At best genes like these might identify 10-15% of pre-eclampsia, so it's relative importance may not be sensational. But it may allow us to study new treatments to prevent or delay the onset of pre-eclampsia and to know which women need closer surveillance."
He said that currently the only real way to halt the condition was to deliver the baby. This can be relatively risk free if the pregnancy is nearing its natural end anyway, but can be risky if the baby is premature.
Infertility- Testing, questions and information

There's a wide range that will "qualify" someone to be considered infertile. For a man, it could be low sperm count, no sperm release, or sperm that are physically incapable of going into the egg on their own. For a women, the list seems to be greater. The range is generally seen as:
You are in your mid-30s or older, have not used birth control for 6 months, and have not been able to become pregnant.
You are in your 20s or early 30s, have not used birth control for a year or more, and have not been able to become pregnant.
How will we be tested?
As a general start-out, both partners are given a general overview. This includes:
Medical History
Physical Exam
Blood and Urine Tests- (LH, prolactin, Progesterone, thyroid, testosterone, and STD's)
There are certain tests specific to each partner that maybe done. Women may be asked to do a postcoital test (checking cervical mucous) and a home LH test. Men may be asked for a semen analysis to check the amount and "capabilities" of his sperm.
Should all the tests not give definite answers a second level of tests could be performed. A general antibody test and karyotyping will be done for both partners. For women a pelvic ultrasound, Hysterosalpingography (HSG), Sonohysterography (SHG), endometrial biopsy and laparoscopy may be performed. For men and ultrasound and/or testicular biopsy may be performed.
It's been studied that for 80% of couples, the cause is either a sperm problem, irregular or no ovulation, or blockage in fallopian tubes. For about 15% of the diagnosed 'infertile' couples, there may be no answers resulting in a diagnosis of unexplained infertility.
The most common causes of infertility have been found to be
Men:
Impaired function of sperm
Impaired delivery of sperm
General health and lifestyle
Environmental exposure
Women:
Fallopian tube damage or blockage
Endometriosis
Ovulation Disorders
Elevated Prolactin
Polycystic Ovary Syndrome (PCOS)
Early Menopause
Uterine Fibroids
Pelvic Adhesions
There are a variety of treatments can be done to help with any diagnosed explanation of infertility.
For men, the solution may be as simple as medication, increased frequency of intercourse or aid in unblocking tubes allowing adequate semen release.
For women, there is a large list of aids:
Clomiphene (Clomid, Serophene)
Human Menopausal Gondrotriphin or hMG (Repronex)
Follicle Stimulating Hormone or FSH (Gonal-F, Bravelle)
Human Chorionic Gonadotripin (Ovidrel, Pregnyl)
Gonadotropin Releasing Hormone
Aromatse Inhibitors
Metformin (Glucophage)
Bromoctrptine (Parlodel)
Assisted Reproductive Technology (IUI, IVF, ICSI)
As with any medical treatment, there can be complications. With fertility medications, the result may be multiple pregnancy, overstimulated ovaries, bleeding or infection, low birth weight, or birth defects.
As with any medical advice, you should only listen to your doctor. They will know the best test, treatment and level of risk for each procedure or aid you may be prescribed.
Additional links and information:
(overview of tests)http://www.webmd.com/infertility-and-reproduction/tc/infertility-tests-overview
(breakdown of tests)http://www.webmd.com/infertility-and-reproduction/guide/infertility-reproduction-diagnosis-tests
(Understanding Infertility) http://www.webmd.com/infertility-and-reproduction/guide/understanding-infertility-treatment
(infertility ‘causes’) http://www.mayoclinic.com/health/infertility/DS00310/DSECTION=causes
(Discussing infertility with a dr) http://www.mayoclinic.com/health/infertility/DS00310/DSECTION=preparing-for-your-appointment
(Treatments and drugs) http://www.mayoclinic.com/health/infertility/DS00310/DSECTION=treatments-and-drugs
(Recent news and updates about infertility) http://www.webmd.com/infertility-and-reproduction/news-features
Feel free to join the discussion on The Board if you have any questions or input or put a comment down below!
RPL- Testing and General Information
What is RPL?
RPL means Repeat/Recurrant Pregnancy Loss. Generally when a woman has had two or more losses confirmed by an OB, they are sent for RPL testing. Many doctors have varying views on when a woman should receive RPL testing. Some may say after “x” many weeks, three losses, or even after a certain age and a certain number of losses. Only your doctor will have the correct answer for you and your situation. If you ever question your doctors decision, it is best to seek a second, professional, opinion.
What will they test for?
Genetic testing
Studies have concluded that about half of all first trimester miscarriages are the result of chromosomal abnormalities. These generally occur on a sporadic basis, meaning that they are random occurrences. They are, however, related to the age of the woman and are more likely to occur with advancing maternal age.
Research suggests that after a couple has had 2 or more unexplained miscarriages, there is a 2-5% risk that one member of the couple is a carrier of a balanced chromosome rearrangement. Chromosomal analysis of the products of conception (the miscarried fetal tissue) and of the woman and her partner may provide additional important information that will affect future reproductive decisions and additional testing recommendations.
Hormonal testing
There are several hormonal imbalances that can contribute to miscarriage rates. These can be evaluated with simple blood tests and treated if present. The recommended hormonal testing will depend up on the symptoms experienced, but may include thyroid, prolactin, follicle stimulating hormone, fasting glucose and insulin levels.
Hematologic and Immunologic Testing
Several blood disorders have been implicated in recurrent miscarriages. Women with abnormal blood clotting may be predisposed to early or late miscarriage and women with high risk personal or family histories should be tested. Women with these disorders have a high success rate when properly treated. Testing and treatment of low risk patients continues to be debated among physicians, however even in these cases, the most common abnormalities should be ruled out.
Uterine Abnormalities.
Distortion of the uterine cavity may be found in approximately 10% to 15% of women with recurrent pregnancy losses.
There are some great online resources to finding out how much testing will cost, a breakdown of each area of testing and what they all mean. Once you get tested and talk to your doctor, you can then move forward. Never start your own treatment based on what is found online. Only your doctor will know the best way to treat you and help you achieve a healthy pregnancy.
(RPL information)http://www.stanfordivf.com/recurrent-pregnancy-loss.html
(RPL Overview) http://emedicine.medscape.com/article/260495-overview
(Should you ask for Genetic Testing?) https://www.dnadirect.com/web/article/testing-for-genetic-disorders/recurrent-pregnancy-loss/50/who-should-consider-testing
(Information on testing cost and breakdown) http://www.fertilityplus.org/faq/miscarriage/rpl.html
Check back for information on Infertility information and testing information and some of the common factors into fertility difficulties.
Feel free to add any questions or comments in the comments section below or in this thread on TTCAL- RPL Blog Post- Link and Discussion/Questions
RPL means Repeat/Recurrant Pregnancy Loss. Generally when a woman has had two or more losses confirmed by an OB, they are sent for RPL testing. Many doctors have varying views on when a woman should receive RPL testing. Some may say after “x” many weeks, three losses, or even after a certain age and a certain number of losses. Only your doctor will have the correct answer for you and your situation. If you ever question your doctors decision, it is best to seek a second, professional, opinion.
What will they test for?
Genetic testing
Studies have concluded that about half of all first trimester miscarriages are the result of chromosomal abnormalities. These generally occur on a sporadic basis, meaning that they are random occurrences. They are, however, related to the age of the woman and are more likely to occur with advancing maternal age.
Research suggests that after a couple has had 2 or more unexplained miscarriages, there is a 2-5% risk that one member of the couple is a carrier of a balanced chromosome rearrangement. Chromosomal analysis of the products of conception (the miscarried fetal tissue) and of the woman and her partner may provide additional important information that will affect future reproductive decisions and additional testing recommendations.
Hormonal testing
There are several hormonal imbalances that can contribute to miscarriage rates. These can be evaluated with simple blood tests and treated if present. The recommended hormonal testing will depend up on the symptoms experienced, but may include thyroid, prolactin, follicle stimulating hormone, fasting glucose and insulin levels.
Hematologic and Immunologic Testing
Several blood disorders have been implicated in recurrent miscarriages. Women with abnormal blood clotting may be predisposed to early or late miscarriage and women with high risk personal or family histories should be tested. Women with these disorders have a high success rate when properly treated. Testing and treatment of low risk patients continues to be debated among physicians, however even in these cases, the most common abnormalities should be ruled out.
Uterine Abnormalities.
Distortion of the uterine cavity may be found in approximately 10% to 15% of women with recurrent pregnancy losses.
There are some great online resources to finding out how much testing will cost, a breakdown of each area of testing and what they all mean. Once you get tested and talk to your doctor, you can then move forward. Never start your own treatment based on what is found online. Only your doctor will know the best way to treat you and help you achieve a healthy pregnancy.
(RPL information)http://www.stanfordivf.com/recurrent-pregnancy-loss.html
(RPL Overview) http://emedicine.medscape.com/article/260495-overview
(Should you ask for Genetic Testing?) https://www.dnadirect.com/web/article/testing-for-genetic-disorders/recurrent-pregnancy-loss/50/who-should-consider-testing
(Information on testing cost and breakdown) http://www.fertilityplus.org/faq/miscarriage/rpl.html
Check back for information on Infertility information and testing information and some of the common factors into fertility difficulties.
Feel free to add any questions or comments in the comments section below or in this thread on TTCAL- RPL Blog Post- Link and Discussion/Questions
What's with all the check-ins?

If you lurk around on TTCAL for a couple days, you'll notice a ton of posts saying there's some sort of check in. They can range from groups of 50 down to a small group of 5 or so.
There are two different kind of check-ins you'll see on the board. One is for larger groups sharing experiences and one is for smaller personal groups who came together rather than doing just "the buddy system".
Women who lost mothers- For any member knowing the difficulties of coping with pregnancy loss or miscarriage without a mother to lean on
Monthly themed group- For the members working toward PgAL and want a new theme each month with badge
Ladies waiting for HCG to drop- For those who know the difficulties of having slowly decreasing betas which may delay your ovulation and start of a fresh cycle
Ladies in waiting- For all those waiting to try again, waiting to ovulate, waiting on testing or start of an IUI or IVF cycle
Mulitple Loss check-in- For any member who has had two losses or more, they are any loss at any point in pregnancy be it a chemical or late loss
There are also groups comprised of smaller numbers who share badges, check-ins, frustrations and give support to each other.
Ten and trying, Rainbow Girls, Naughty Nine, Sweet Mix, 8 Ladies Hoping For Luck, Beyond Appearances and Hope Buddies
Those are most of the one's you'll see pop up. If you'd like to start your own group or ask to join one, don't be afraid. You'll find so many wonderful members looking to support one another.
Please help in
Welcoming our newest admins for the blog!
Noah-bear
Laurakat81
Thanks for volunteering girls!
TTCALers, if you have any blog related questions, please page them on TTCAL.
Clomid Monitoring thread
As this thread seen on the Bump describes, it is important to be monitored when you take Clomid...
http://community.thenest.com/cs/ks/forums/37115533/ShowThread.aspx?MsdVisit=1
Thanks to those who suggested I post this here.
http://community.thenest.com/cs/ks/forums/37115533/ShowThread.aspx?MsdVisit=1
Thanks to those who suggested I post this here.
You know you're TTC when....
One night on TTCAL, the ladies and myself made a list of how you know when you're TTC...here's what we came up with.
You know you're TTC when...
..you're actually dreading FWP tonight
..you have absolutely no idea what the date is, but you know exactly what CD or DPO you are
..you have to hold your pee for 3 hours to test
..when the most action you get (other than FWP) is checking your CM...daily
..you're constantly calculating your EDD based on time of O, and you don't need a calender
..you carry around OPKs in your pocket and wait for 2 PM
..you've gotten *really* good at fingering yourself
..when you schedule events based around peak O times
..you don't drink after 9 PM because you want really great test pee for a 2 PM OPK
..when you are pissed with DH and make up with him just in time for FWP...where any other time you'd be holding a grudge and not giving him any!
..you constantly feel yourself up to see if there are any twinges or pain
..you measure time by cycles or by how many weeks you would have been pregnant at the time
..you check the price of HPTs every time you're at a store
..You get excited about CM and have to avoid telling people about when you finally see those EWs!
..you inadvertently grab your boobs at work for a quick tenderness check and enough people notice you start to get a few eyebrows raised
..your co-workers know when it's your 2ww because you won't work out with them
..when your friends figure out you're on 2ww because you won't drink with them.
..you cannot wait to get up in the morning to temp and once you do, you can't go back to sleep because you are analyzing you patterns on FF
..When you read ETC as TTC and pom as porn
..when you are chatting online with someone and using bump abbreviations with them...and they aren't on the bump
..when you don't have to look or focus to POAS
..when you schedule sex a week in advance down to the time of day
..when you take an OPK at the stalls at work and wait the 5 minutes for the results
..when DH starts to tell others about your FWP
..DH understands what FWP, CD, DPO, OPK, HPT, EWCM, AF, CBEFM, BFP, BFN, EOD, and TTCAL all mean
..when you POAS much too early in your cycle and still throughout the week check it to see if it mysteriously changed to positive
..when you have a calender with bunny stickers on it for the days you need some action, and DH regularly checks the calender
Hope you enjoyed, and you can probably relate! Thanks CashewsMommy for starting this and to the rest of the TTCAL ladies for contributing.
You know you're TTC when...
..you're actually dreading FWP tonight
..you have absolutely no idea what the date is, but you know exactly what CD or DPO you are
..you have to hold your pee for 3 hours to test
..when the most action you get (other than FWP) is checking your CM...daily
..you're constantly calculating your EDD based on time of O, and you don't need a calender
..you carry around OPKs in your pocket and wait for 2 PM
..you've gotten *really* good at fingering yourself
..when you schedule events based around peak O times
..you don't drink after 9 PM because you want really great test pee for a 2 PM OPK
..when you are pissed with DH and make up with him just in time for FWP...where any other time you'd be holding a grudge and not giving him any!
..you constantly feel yourself up to see if there are any twinges or pain
..you measure time by cycles or by how many weeks you would have been pregnant at the time
..you check the price of HPTs every time you're at a store
..You get excited about CM and have to avoid telling people about when you finally see those EWs!
..you inadvertently grab your boobs at work for a quick tenderness check and enough people notice you start to get a few eyebrows raised
..your co-workers know when it's your 2ww because you won't work out with them
..when your friends figure out you're on 2ww because you won't drink with them.
..you cannot wait to get up in the morning to temp and once you do, you can't go back to sleep because you are analyzing you patterns on FF
..When you read ETC as TTC and pom as porn
..when you are chatting online with someone and using bump abbreviations with them...and they aren't on the bump
..when you don't have to look or focus to POAS
..when you schedule sex a week in advance down to the time of day
..when you take an OPK at the stalls at work and wait the 5 minutes for the results
..when DH starts to tell others about your FWP
..DH understands what FWP, CD, DPO, OPK, HPT, EWCM, AF, CBEFM, BFP, BFN, EOD, and TTCAL all mean
..when you POAS much too early in your cycle and still throughout the week check it to see if it mysteriously changed to positive
..when you have a calender with bunny stickers on it for the days you need some action, and DH regularly checks the calender
Hope you enjoyed, and you can probably relate! Thanks CashewsMommy for starting this and to the rest of the TTCAL ladies for contributing.
Subscribe to:
Posts (Atom)