Please take note that the TTCAL BLOG has a NEW HOME!
Please visit at http://ttcalblog.wordpress.com for any and all new updates!
See you there!


Incompetent Cervix Facts
Thanks to rlajambe for writing this very informative and helpful blog post!!!
What is incompetent Cervix (IC)?
Incompetent cervix (IC) is essential a weak cervix. Mainly occurring in the 2nd trimester, the weight of the baby causes the cervix to dilate prematurely and this can result in premature labour (PTL). IC is characterized by dilation in the absence of contractions.
What is cervical insufficiency?
Cervical insufficiency is having little to no cervix. Some women are born with little to no cervix due to a congenital anomaly. Surgery can also be a main reason for cervical insufficiency. A cone biopsy or a cervical surgery for cancer can result in part of the cervix being compromised and cervical insufficiency.
How is it diagnosed?
Unfortunately, unless dilation is detected during a routine ultrasound, IC is very hard to diagnose. Some women lose multiple babies in the 2nd trimester without a reason. Generally, three losses in the 2nd trimester with premature labour are deemed to be IC. However, doctors have started to perform more cervical monitoring for women with suspected IC.
What treatment options are there for IC?
Cervical cerclage (aka cervical stitches) – stitches are placed to hold the cervix closed and prevent cervical shortening. There are two main types:
Preventative cerclage – placed at around the 12-13th week of gestation. When a diagnosis of IC has been made during a previous pregnancy, your OB will likely recommend a cerclage at the end of the 1st trimester. The success rate is about 90-95%.
Emergent cerclage – placed during the 2nd trimester after dilation has already started. This type is usually due to the discovery of IC that was not known. The success rate is lower (40-60%) than the preventative cerclage, but many women are successful with this technique. Also, most doctors will not perform an emergent cerclage after 23 weeks due to the risk of premature rupture of membranes and possible infection.
Bed rest – By placing the women on bed rest, the baby’s weight is taken off the cervix and the cervix is less likely to dilate. The bed rest period will vary from one women to another usually depending on cervical length through the course of the pregnancy.
Progesterone -Some women experience contractions even after the cerclage is placed. Progesterone gels or P17 injections (17 alpha-hydroxyprogesterone caproate) are intended to prevent the onset of PTL.
Cervical length monitoring – The length of the cervix will be measured and examined to check for shortening and/or funneling. Transvaginal ultrasound generally gives more reliable measurements than transabdominal ultrasound.
Your doctor may recommend one or all of these treatments depending on your specific situation.
Dr. Google told me that there are different methods of cerclage. What is the difference between them?
There are two main methods of cerclage. Each has advantages and disadvantages.
Transvaginal Cerclage (TVC) - This method is the most common. It is essentially placing sutures onto the cervix to hold it closed. There are several techniques of how the stitches are placed (McDonald’s, Shiradkor, etc.); however, all have approximately the same success rate. Different doctors have preferences for specific techniques.
Advantages
- the sutures can removed from the cervix and allow for a vaginal delivery
- no incisions are needed as the sutures are placed through the vaginal opening
Disadvantages
- not suitable for women with cervical insufficiency
Transabdominal Cerclage (TAC)- This method is usually reserved for women with a failed transvaginal cerclage or those with cerclage insufficiency. Sutures and surgical mesh are placed internally (inside the abdomen) to close the cervical opening.
Advantages
- higher success rate than transvaginal
Disadvantages
- makes vaginal delivery impossible, you must have a C-section
- requires laproscopic surgeries during pregnancy to be placed
- often not available unless a TVC has already failed
Why doesn’t my OB place the cerclage as soon as I get a BFP?
Viability. You OB will want to ensure that the pregnancy is viable before placing the cerclage. Otherwise, they will have to perform two surgeries (placement and removal). Unfortunately, women with IC still have same risk of a 1st trimester loss as any other woman does.
I had IC with my twins. Will it happen again with another pregnancy?
Not necessarily. Some women who have IC with multiples go on to have normal pregnancies with singletons. However, there is no way to know for sure. Some doctors will take the “wait and see” approach, but this can be risky. Finding a doctor that will perform the cerclage preventatively can be difficult, but is highly recommended.
What can I do while we’re TTC?
Get the right doctor – The right OB will make all the difference in having a successful pregnancy. Find an OB with experience with IC and cerclage. You will need to have your doctor in place before you get pregnant, as you will need to start your appointments sooner than most women. Discuss your plan with your OB before you get pregnant. Be clear about what restrictions will be in place during the pregnancy.
For those who live in more rural areas, you may have look to a major city to find the right doctor. You want someone who performs cerclages on at least a semi-regular basis, not the OB that does one cerclage a year or less.
Get the right insurance and get your finances in order – You know that you will be high-risk next time out, make sure you have the financial resources to cover all the possible expenses that may arise. Bed rest (with no income) and extra doctor visits are not cheap.
Get in shape physically – You can’t make your cervix any stronger, but you can get everything else stronger. Being in shape physically will help to prevent any other complications, like gestational diabetes or high blood pressure. You have enough to manage with IC.
Consider talking to a therapist – Your loss can be very difficult to process. Therapy can help you work through all the emotional issues of your loss and a subsequent pregnancy.
Recurrent Pregnancy Loss (RPL) Testing
Pregnancy loss alone is devastating. Not knowing why it occurs even once is heartbreaking. To continue to experience loss after loss causes anxiety, depression and fear. Recurrent pregnancy loss is typically defined as 3+ consecutive losses, while some practitioners may Dx RPL as 2 consecutive losses.
One thing I ran into personally, was I had two early miscarriages and then an ectopic- some doctors may not consider this RPL because ectopics are either flukes or caused by tubal factors, not necessarily in the same department as another type of loss. My old OB did not feel as though I need RPL testing, whereas my current OB and RE did. Depending on the types of losses you've had, your doctor may order a couple, a handful or all of the testing listed below.
Bottom line is you need to advocate for what you feel is right. RPL testing can be very expensive (I've listed prices my insurance was billed FYI, but obviously prices and benefits will vary), emotionally exhausting and may still not provide you with answers. Below are some tests you may request or discuss with your medical practitioner. I decided not to include normal lab values because one lab's 'normal' may be another lab's 'abnormal'.
One thing I ran into personally, was I had two early miscarriages and then an ectopic- some doctors may not consider this RPL because ectopics are either flukes or caused by tubal factors, not necessarily in the same department as another type of loss. My old OB did not feel as though I need RPL testing, whereas my current OB and RE did. Depending on the types of losses you've had, your doctor may order a couple, a handful or all of the testing listed below.
Bottom line is you need to advocate for what you feel is right. RPL testing can be very expensive (I've listed prices my insurance was billed FYI, but obviously prices and benefits will vary), emotionally exhausting and may still not provide you with answers. Below are some tests you may request or discuss with your medical practitioner. I decided not to include normal lab values because one lab's 'normal' may be another lab's 'abnormal'.
- Hormonal Factors Tests (prices may vary from $50-300 per test): This includes prolactin, thyroid and progesterone. Other hormones that may be checked (as part of an IF work-up, some tests may be cycle day sensitive) are estradiol, testosterone, LH and FSH.
- An imbalance with one or more hormone may warrant treatment depending on the Dx. Depending on hormonal imbalance an ultrasound may also be ordered to make a firm Dx (PCOS, DOR)
- Blood Clotting Disorders- typically treated with some type of blood thinner (baby aspirin, heparin, lovenox)
- homocysteine/MTHFR
- Prothrombin gene
- Protein C&S
- Antithrombin III
- Factor V Leiden
- Fibrinogen
- PT/PTT (INR)
- Structural Factors Tests: These tests are conducted to determine the size and shape of your uterus as well as checking the uterine wall in hopes it is free of scarring, polyps, fibroids or a septum- all of which can affect implantation. Tests to check the integrity of your tubes may also be ordered if one or more of your losses were ectopic, or if you are at higher risk for one.
- SHG (sonohysterogram) ($300-ish): This test is conducted by inserting a catheter through your cervix to push saline into the uterine cavity. Simultaneously, your doctor will also be performing a transvaginal ultrasound to get a visual of your uterus. This test can identify if there’s abnormalities in your uterus (listed above). If there are concerns about the uterus, a hysteroscopy or laparoscopy may be performed to fix and further Dx the issue.
- HSG (hysterosalpingogram) ($500-ish): This test is typically performed in your local hospital’s X-ray lab by an X-ray tech, and sometimes your doctor depending on how their practice handles this procedure. Similar to an SHG, a catheter is inserted through your cervix, except this test requires dye to get an adequate picture of your tubes. Sometimes, simply performing this test may unblock tubes if there’s a blockage while other situations may require surgery.
- Uterine Lining Test/ Endometrial Biopsy: While this test is considered obsolete by some in the medical community (results may vary from tech to tech reading doing the biopsy, which may not give accurate results), it can still be an important piece of the puzzle, especially if you’re dealing with possible luteal phase defect (LPD) or spotting for more than a couple days during your LP.
- This test is typically performed in the office after CD 21 (be SURE you have ovulated, as this test is checking your uterine lining for implantation). To get an accurate and reliable reading, it is typically recommended for this test to be performed two cycles for comparison to make a firm Dx.
- If the uterine lining is ‘out of phase’ (2+ days... meaning you’re 7dpo and your biopsy is showing 9dpo, your body may not be adequately using hormones to build your uterine lining) treatments of clomid/femara, hCG trigger and/or booster and progesterone supplementation may be used for Tx.
- I do want to mention that if the endo biopsy does leave you with a LPD Dx, to ask your doctor about what type of defect it is. Click HERE to read more about the different types and causes. LPD is a controversial Dx in the medical community, about 50/50- if you are concerned about your LP and your doctor does not believe it's an issue, seek a second opinion.
- Tests for Chromosomal Causes:
- Pathology from D&C/D&E ($480- pathology only): this will show if the cause of your loss was from a chromosomal abnormality or not. Most chromosomal abnormalities found are not typical to repeat in the future.
- Genetic testing (saliva testing $960 for MH and I) on one or both partners- This may consist of blood or saliva tests. Some cultural groups may be at higher risk/genetic carriers for certain chromosomal defects.
- Karyotyping ($2300 for MH and I): Blood test to be performed on you and your partner to check for translocations (normal number of genes, but are joined together abnormally) Tests for
- Immunologic Causes: This is one area that seems to not have as much research on all areas of testing, some are controversial and some are routine- and that I admittedly do not know much about. If you have more information I can add to this section, please feel free to leave a comment, message me on the bump or page me on TTCAL.
- Anti cardiolipin antibodies (ACA)
- Anti-nuclear antibodies (ANA)
- Anti-thyroid antibodies (ATA)
- Anti-Ovarian Antibodies (AOA)
- Anti-Sperm Antibodies (ASA)
- Anti-phospholipid antibodies (APA)
- Leukocyte Antibody Detection (LAD)
- Lupus anticoagulant (LAC)
- Embryo Toxic Factor (ETF)
- NK activation assay (NKa)
- reproductive immuno-phenotype (RIP)
The Scoop on Ectopic Pregnancies
Looking back over the blog I realized that we have not posted anything about Ectopic Pregnancies yet we have quite a few ladies on the board that have experienced them. So let's go over what a Ectopic Pregnancy is and sign and symptoms to look for. I personally have not experienced one so if any of the ladies that have would like to chime in on anything please get a hold of me.
What is a ectopic pregnancy?
An ectopic pregnancy, or eccysis, is a complication of pregnancy in which the embryo implants outside the uterine cavity. With rare exceptions, ectopic pregnancies are not viable. Furthermore, they are dangerous for the mother, since internal haemorrhage is a life threatening complication. Most ectopic pregnancies occur in the Fallopian tube (so-called tubal pregnancies), but implantation can also occur in the cervix, ovaries, and abdomen. An ectopic pregnancy is a potential medical emergency, and, if not treated properly, can lead to death.
About 1% of pregnancies are in an ectopic location with implantation not occurring inside of the womb, and of these 98% occur in the Fallopian tubes.
In a typical ectopic pregnancy, the embryo adheres to the lining of the fallopian tube and burrows into the tubal lining. Most commonly this invades vessels and will cause bleeding. This intratubal bleeding hematosalpinx expels the implantation out of the tubal end and is a common type of miscarriage. There is no inflammation of the tube in ectopic pregnancy. The pain is caused by prostaglandins released at the implantation site, and by free blood in the peritoneal cavity, which is a local irritant. Sometimes the bleeding might be heavy enough to threaten the health or life of the woman. Usually this degree of bleeding is due to delay in diagnosis, but sometimes, especially if the implantation is in the proximal tube (just before it enters the uterus), it may invade into the nearby Sampson artery, causing heavy bleeding earlier than usual.
If left untreated, about half of ectopic pregnancies will resolve without treatment. These are the tubal miscarriages. The advent of methotrexate* treatment for ectopic pregnancy has reduced the need for surgery; however, surgical intervention is still required in cases where the Fallopian tube has ruptured or is in danger of doing so. This intervention may be laparoscopic or through a larger incision, known as a laparotomy.
*Methotrexate, abbreviated MTX and formerly known as amethopterin, is an antimetabolite and antifolate drug. It is used in treatment of cancer, autoimmune diseases, and ectopic pregnancy.
I've suffered an ectopic pregnancy, but my hCG keeps rising.. what could be going on?
There is a chance that you are still retaining tissue from your loss, you may be going through what is called a heterotopic pregnancy, or you may be going through a persstent ectopic pregnancy, either way you should be in contact with you doctor about your concerns for testing and monitoring.
Although rare, heterotopic pregnancies are becoming more common, likely due to increased use of IVF. The survival rate of the uterine fetus of an ectopic pregnancy is around 70%.
Successful pregnancies have been reported from ruptured tubal pregnancy continuing by the placenta implanting on abdominal organs or on the outside of the uterus.
Persistent ectopic pregnancy
A persistent ectopic pregnancy refers to the continuation of trophoplastic growth after a surgical intervention to remove an ectopic pregnancy. After a conservative procedure that attempts to preserve the affected fallopian tube such as a salpingotomy, in about 15-20% the major portion of the ectopic growth may have been removed, but some trophoblastic tissue, perhaps deeply embedded, has escaped removal and continues to grow, generating a new rise in hCG levels. After weeks this may lead to new clinical symptoms including bleeding. For this reason hCG levels may have to be monitored after removal of an ectopic to assure their decline, also methotrexate can be given at the time of surgery prophylactically.
What are some signs and symptoms I should be looking for if I do become pregnant?
Early symptoms are either absent or subtle. Clinical presentation of ectopic pregnancy occurs at a mean of 7.2 weeks after the last normal menstrual period, with a range of 5 to 8 weeks. Later presentations are more common in communities deprived of modern diagnostic ability.
Early signs include:
More severe internal bleeding may cause:
What causes Ectopic Pregnancies?
There are a number of risk factors for ectopic pregnancies. However, in as many as one third to one half of ectopic pregnancies, no risk factors can be identified. Risk factors include: pelvic inflammatory disease, infertility, use of an intrauterine device (IUD), tubal surgery, intrauterine surgery (e.g. D&C), smoking, previous ectopic pregnancy, and tubal ligation.
Will experiencing an Ectopic Pregnancy lead to fertility problems in the future?
Fertility following ectopic pregnancy depends upon several factors, the most important of which is a prior history of infertility. The treatment choice, whether surgical or nonsurgical, also plays a role. For example, the rate of intrauterine pregnancy may be higher following methotrexate compared to surgical treatment.
*** All this information was obtained by certified sources on Wikipedia.org
What is a ectopic pregnancy?
An ectopic pregnancy, or eccysis, is a complication of pregnancy in which the embryo implants outside the uterine cavity. With rare exceptions, ectopic pregnancies are not viable. Furthermore, they are dangerous for the mother, since internal haemorrhage is a life threatening complication. Most ectopic pregnancies occur in the Fallopian tube (so-called tubal pregnancies), but implantation can also occur in the cervix, ovaries, and abdomen. An ectopic pregnancy is a potential medical emergency, and, if not treated properly, can lead to death.
About 1% of pregnancies are in an ectopic location with implantation not occurring inside of the womb, and of these 98% occur in the Fallopian tubes.
In a typical ectopic pregnancy, the embryo adheres to the lining of the fallopian tube and burrows into the tubal lining. Most commonly this invades vessels and will cause bleeding. This intratubal bleeding hematosalpinx expels the implantation out of the tubal end and is a common type of miscarriage. There is no inflammation of the tube in ectopic pregnancy. The pain is caused by prostaglandins released at the implantation site, and by free blood in the peritoneal cavity, which is a local irritant. Sometimes the bleeding might be heavy enough to threaten the health or life of the woman. Usually this degree of bleeding is due to delay in diagnosis, but sometimes, especially if the implantation is in the proximal tube (just before it enters the uterus), it may invade into the nearby Sampson artery, causing heavy bleeding earlier than usual.
If left untreated, about half of ectopic pregnancies will resolve without treatment. These are the tubal miscarriages. The advent of methotrexate* treatment for ectopic pregnancy has reduced the need for surgery; however, surgical intervention is still required in cases where the Fallopian tube has ruptured or is in danger of doing so. This intervention may be laparoscopic or through a larger incision, known as a laparotomy.
*Methotrexate, abbreviated MTX and formerly known as amethopterin, is an antimetabolite and antifolate drug. It is used in treatment of cancer, autoimmune diseases, and ectopic pregnancy.
I've suffered an ectopic pregnancy, but my hCG keeps rising.. what could be going on?
There is a chance that you are still retaining tissue from your loss, you may be going through what is called a heterotopic pregnancy, or you may be going through a persstent ectopic pregnancy, either way you should be in contact with you doctor about your concerns for testing and monitoring.
Heterotopic pregnancy
In rare cases of ectopic pregnancy, there may be two fertilized eggs, one outside the uterus and the other inside. This is called a heterotopic pregnancy. Often the intrauterine pregnancy is discovered later than the ectopic, mainly because of the painful emergency nature of ectopic pregnancies. Since ectopic pregnancies are normally discovered and removed very early in the pregnancy, an ultrasound may not find the additional pregnancy inside the uterus. When hCG levels continue to rise after the removal of the ectopic pregnancy, there is the chance that a pregnancy inside the uterus is still viable. This is normally discovered through an ultrasound.Although rare, heterotopic pregnancies are becoming more common, likely due to increased use of IVF. The survival rate of the uterine fetus of an ectopic pregnancy is around 70%.
Successful pregnancies have been reported from ruptured tubal pregnancy continuing by the placenta implanting on abdominal organs or on the outside of the uterus.
Persistent ectopic pregnancy
A persistent ectopic pregnancy refers to the continuation of trophoplastic growth after a surgical intervention to remove an ectopic pregnancy. After a conservative procedure that attempts to preserve the affected fallopian tube such as a salpingotomy, in about 15-20% the major portion of the ectopic growth may have been removed, but some trophoblastic tissue, perhaps deeply embedded, has escaped removal and continues to grow, generating a new rise in hCG levels. After weeks this may lead to new clinical symptoms including bleeding. For this reason hCG levels may have to be monitored after removal of an ectopic to assure their decline, also methotrexate can be given at the time of surgery prophylactically.
What are some signs and symptoms I should be looking for if I do become pregnant?
Early symptoms are either absent or subtle. Clinical presentation of ectopic pregnancy occurs at a mean of 7.2 weeks after the last normal menstrual period, with a range of 5 to 8 weeks. Later presentations are more common in communities deprived of modern diagnostic ability.
Early signs include:
- Pain in the lower abdomen, and inflammation (pain may be confused with a strong stomach pain, it may also feel like a strong cramp).
- Pain while urinating.
- Pain and discomfort, usually mild. A corpus luteum on the ovary in a normal pregnancy may give very similar symptoms.
- Vaginal bleeding, usually mild. An ectopic pregnancy is usually a failing pregnancy and falling levels of progesterone from the corpus luteum on the ovary cause withdrawal bleeding. This can be indistinguishable from an early miscarriage or the 'implantation bleed' of a normal early pregnancy.
- Pain while having a bowel movement.
- External bleeding is due to the falling progesterone levels.
- Internal bleeding is due to hemorrhage from the affected tube.
More severe internal bleeding may cause:
- Lower back, abdominal, or pelvic pain.
- Shoulder pain. This is caused by free blood tracking up the abdominal cavity and irritating the diaphragm, and is an ominous sign.
- There may be cramping or even tenderness on one side of the pelvis.
- The pain is of recent onset, meaning it must be differentiated from cyclical pelvic pain, and is often getting worse.
What causes Ectopic Pregnancies?
There are a number of risk factors for ectopic pregnancies. However, in as many as one third to one half of ectopic pregnancies, no risk factors can be identified. Risk factors include: pelvic inflammatory disease, infertility, use of an intrauterine device (IUD), tubal surgery, intrauterine surgery (e.g. D&C), smoking, previous ectopic pregnancy, and tubal ligation.
Will experiencing an Ectopic Pregnancy lead to fertility problems in the future?
Fertility following ectopic pregnancy depends upon several factors, the most important of which is a prior history of infertility. The treatment choice, whether surgical or nonsurgical, also plays a role. For example, the rate of intrauterine pregnancy may be higher following methotrexate compared to surgical treatment.
*** All this information was obtained by certified sources on Wikipedia.org
Interesting Article
Pressure to Father Child
Please take some time to read this article.
Summary taken from this post on the Infertility board on thebump.com
Please take some time to read this article.
Short version: Timed sex can lead to issues with men's libido and the researchers don't recommend more than a few months of timed sex. Some men also are more prone to erectile disfunction and straying after prolonged timed sex.
____________________________________________________________________________
Long version:
"Any couple trying for a baby is told that timing is everything. But pressure to perform when their partner is at her most fertile drives men away, according to research.
One in ten men has had an affair because of the pressure of rigorously timed sessions, while four out of ten claimed it made them impotent.
More than 400 men took part in the study, which found the pressure to conceive a baby caused men acute stress.
Fertility experts routinely tell couples to time intercourse to coincide with the window when a woman is ovulating. There are even highly sensitive devices designed to help couples work out – down to the minute – when she is at her most fertile.
But as the number of timed sex sessions increased so did the men’s level of stress, according to the research carried out in South Korea. None of the men in the study had ever had sexual problems.
The finding supports several previous studies showing that men who are under stress produce less testosterone, which has an effect on their libido.The authors suggested couples should be made aware of these risks and attempt timed sessions for no longer than three months at a time, with breaks for a few months in between.
Timed intercourse seems to impose a substantial degree of stress on male partners, inducing erectile dysfunction and, in some cases, causing them to seek extramarital sex,’ they wrote in the Journal Of Andrology. Andrology is the branch of medicine concerned with diseases in men, especially the reproductive organs.
They added: ‘It is clear that the greater instances of timed intercourse trials, the more incidences of erectile dysfunction and extramarital sex and the greater the desire to avoid sex with the intended partner.’ All the couples in the study had been trying to conceive naturally for a year.
The authors noted that having to sleep with their partner at a specific time ‘becomes a burden and is carried out as a job to be done, which imposes further stress’. They believe that higher levels of cortisol, the stress hormone, being produced by the body was to blame for lower testosterone.
Professor Allan Pacey, a senior lecturer in andrology at the University of Sheffield, said: ‘I’m glad someone has studied this, as the single biggest concern for men – usually when their partner is not in the room – is that they really find it a struggle when their partners are obsessed with timing.
‘While it is useful for couples to be aware of the fertile window, obsessing about it is not helpful at all. Men are being phoned up at three in the afternoon and told that the green light is on and they have to come home immediately.’
Professor Pacey, also chairman of the British Fertility Society, added: ‘If couples are having regular sex two or three times a week, they will hit the fertile window.’
In the UK the age limit for free IVF treatment is to be raised to
42. Currently only women up to 39 are allowed three free rounds of NHS fertility treatment. Draft guidelines being put out for consultation by the rationing body Nice could allow 8,000 more women in their early 40s to benefit. At present they have to pay up to £5,000 per treatment."
Summary taken from this post on the Infertility board on thebump.com
OPKs: Positive or Negative?
One of the most asked questions on TTCAL is "How do I know if my OPK is positive or negative?". It can be hard to tell sometimes. Hopefully this blog post can help clear up any confusion and make your TTCAL journey a little easier.
First let's recap what OPKs are and how they work. OPK is short for Ovulation Prediction Kits.These tests pick up the Luteinizing Hormone (LH) surge that is produced just before ovulation. Just like a Home Pregnancy Tests (HPT), these tests come in different forms; strips, cassettes or midstream.
The best time of day to test would be late afternoon. Anything from 2pm is advisable until about 8pm. Reason being that LH is more concentrated in your urine later in the day, as opposed to early morning. FMU is not recommended when testing with an OPK.
Try limiting fluid intake before testing, as well as holding your urine for 2-3 hours before.
If you are taking Clomid/Fertomid it is recommended that you do not start testing until a day or two after your last pill. Sometimes these fertility pills can cause a false positive.
How long do I test for?You will need to test until you get your positive result i.e. detecting your LH surge. This can vary from 4 days to 10 days depending on how long your cycles are. The shorter your cycle the less tests you will need. You would most likely “see” your surge within 4-5 days from testing.
What is a positive, I have two lines???
This can be a bit tricky. Since an OPK does not “read” the same as a HPT. A line is NOT always a positive line on an OPK. You will need your test line to be darker than or as dark as the control line. A faint test line only indicates some LH being picked up, not your surge. So keep testing until your test line gets as dark as the control line.
I have my positive, now what?
Once you get detect your surge, you can ovulate 12 – 36 hours after your positive result. (Bear in mind you can wait as long as 48 hours.) Intercourse (BD-Baby Dancing) can take place the day of the positive OPK; you can skip the next day and BD after that. Although you shouldn’t really miss more than two consecutive days of intercourse when Trying to Conceive (TTC). Of course there is nothing wrong with every day either as long as your partner does not have sperm health issues. If you are tracking your Basal Body Temperature (BBT), keep BD until you confirm your thermal shift.
All above Info came from Making Babies
And since it is always easier to compare your OPKs to a picture, here are a few diagrams and pictures of different types of tests that will make it easier to figure out if your OPK is positive or negative.


 See how the bottom one is as dark (if not a little darker) than the control line. That is a positive result. The 2PM test is not quite positive but almost there.
See how the bottom one is as dark (if not a little darker) than the control line. That is a positive result. The 2PM test is not quite positive but almost there.
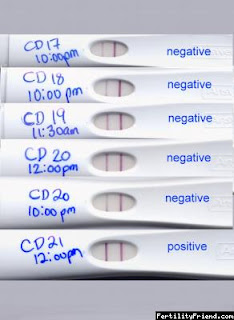
Another example of an OPK test, same principle.. not positive until the test line is as dark or darker than the control line.


First let's recap what OPKs are and how they work. OPK is short for Ovulation Prediction Kits.These tests pick up the Luteinizing Hormone (LH) surge that is produced just before ovulation. Just like a Home Pregnancy Tests (HPT), these tests come in different forms; strips, cassettes or midstream.
When is the best time to test?
This all depends on how long your cycles are. Use the following table as a guide line as to when to start testing.
This all depends on how long your cycles are. Use the following table as a guide line as to when to start testing.
| Cycle | Start Day |
| 21 | 5 |
| 22 | 5 |
| 23 | 6 |
| 24 | 7 |
| 25 | 8 |
| 26 | 9 |
| 27 | 10 |
| 28 | 11 |
| 29 | 12 |
| 30 | 13 |
| 31 | 14 |
| 32 | 15 |
| 33 | 16 |
| 34 | 17 |
| 35 | 18 |
| 36 | 19 |
| 37 | 20 |
| 38 | 21 |
| 39 | 22 |
The best time of day to test would be late afternoon. Anything from 2pm is advisable until about 8pm. Reason being that LH is more concentrated in your urine later in the day, as opposed to early morning. FMU is not recommended when testing with an OPK.
Try limiting fluid intake before testing, as well as holding your urine for 2-3 hours before.
If you are taking Clomid/Fertomid it is recommended that you do not start testing until a day or two after your last pill. Sometimes these fertility pills can cause a false positive.
How long do I test for?You will need to test until you get your positive result i.e. detecting your LH surge. This can vary from 4 days to 10 days depending on how long your cycles are. The shorter your cycle the less tests you will need. You would most likely “see” your surge within 4-5 days from testing.
What is a positive, I have two lines???
This can be a bit tricky. Since an OPK does not “read” the same as a HPT. A line is NOT always a positive line on an OPK. You will need your test line to be darker than or as dark as the control line. A faint test line only indicates some LH being picked up, not your surge. So keep testing until your test line gets as dark as the control line.
I have my positive, now what?
Once you get detect your surge, you can ovulate 12 – 36 hours after your positive result. (Bear in mind you can wait as long as 48 hours.) Intercourse (BD-Baby Dancing) can take place the day of the positive OPK; you can skip the next day and BD after that. Although you shouldn’t really miss more than two consecutive days of intercourse when Trying to Conceive (TTC). Of course there is nothing wrong with every day either as long as your partner does not have sperm health issues. If you are tracking your Basal Body Temperature (BBT), keep BD until you confirm your thermal shift.
All above Info came from Making Babies
And since it is always easier to compare your OPKs to a picture, here are a few diagrams and pictures of different types of tests that will make it easier to figure out if your OPK is positive or negative.

Another example of an OPK test, same principle.. not positive until the test line is as dark or darker than the control line.
Left (Not Positive), Right (Positive)
Then of course the lovely Smiley face!
Subscribe to:
Posts (Atom)